


A person in Euless or Dallas lands on this question at a rough moment. A spouse has started hiding alcohol. A college student cannot stop using pills. A working professional is trying to hold a job together while panic, depression, or drug use keeps getting worse. Then the search results start throwing out terms like inpatient, residential, PHP, and IOP.
That confusion is normal.
Individuals are not trying to become experts in treatment language. They are trying to answer one urgent question. What kind of help gives the best chance of getting better without choosing something that is either too little or more restrictive than necessary?
The right answer is rarely the most extreme option or the most convenient one. It is the level of care that fits the person’s actual risk, daily stability, and support system. Someone with serious withdrawal risk or an unsafe home environment may need the structure of inpatient care. Someone with stable housing, family support, and the ability to participate consistently may do very well in outpatient treatment.
This guide gives a plain-English framework for the difference between inpatient and outpatient, when each makes sense, how people move between levels of care, and what families in the Dallas-Fort Worth area should think about before making a decision.
Table of Contents
- Navigating Your Path to Recovery
- Defining Addiction Treatment Settings
- A Detailed Comparison of Inpatient vs Outpatient Treatment
- Matching the Treatment Level to Your Needs
- Understanding Costs and Insurance Coverage in Texas
- How to Transition Between Levels of Care
- Take the First Step Toward Recovery in Euless and Dallas
Navigating Your Path to Recovery
A common situation looks like this. A family has spent weeks arguing about whether someone “really needs rehab.” The person needing help insists they cannot disappear for a month. The family worries that staying at home will lead to more using, more lying, and another crisis.
Both sides often react to something real.
The person needing help may be afraid of losing work, school, privacy, or control. The family may have already watched several attempts at cutting back fail. By the time the search for treatment begins, nobody feels calm or objective.
That is why the difference between inpatient and outpatient matters so much. This is not just a vocabulary lesson. It is a decision about safety, structure, and realistic follow-through.
Some people need separation from daily triggers. Others need to stay engaged in normal life while learning how to handle cravings, stress, and mental health symptoms in real time. A treatment plan only works if it matches what the person can complete.
The best level of care is not the one that sounds strongest. It is the one that fits the person well enough for them to stay in treatment and use it.
The decision gets easier when the terms are stripped down to what they mean in day-to-day life. Once that happens, the choice becomes far less mysterious.
Defining Addiction Treatment Settings
Most addiction treatment falls under two broad umbrellas. Inpatient care and outpatient care.
That sounds simple, but many people get tripped up because each umbrella includes several different levels of support. Those levels matter.
Inpatient care
Inpatient treatment means the person lives at the treatment facility or in a hospital-based setting for a period of time. Daily life becomes highly structured. Staff manage the schedule, the environment, and the immediate response to crises.
Two forms are common.
Medically supervised detox is short-term care for withdrawal management. This is the level used when stopping alcohol, opioids, benzodiazepines, or other substances could become medically risky or destabilizing.
Residential treatment goes beyond detox. The person stays on site and participates in therapy, recovery activities, and daily routines in a controlled setting. This is frequently the right call when relapse risk is high, the home environment is unstable, or mental health symptoms are severe enough to interfere with basic functioning.
A major study covering 318,924 substance use disorder treatment cases found that outpatient care made up 84.6% of cases, while residential treatment represented 15.4%, yet completion was lower in outpatient at 51.9% compared with 64.5% in residential. The same analysis found residential clients were over three times more likely to complete treatment even after controlling for other factors. The full breakdown appears in this analysis of residential versus outpatient treatment in the US.
That is the key lesson. More common does not always mean better matched.
Outpatient care
Outpatient treatment means the person lives at home and travels to treatment on a schedule. This category ranges from structured to light-touch.
The main levels are:
Partial Hospitalization Program or PHP
PHP is the most intensive outpatient level used after detox or residential care, or for people who need strong daily support without overnight stay. Verified guidance describes PHP as involving significant daily hours, multiple days a week, in common treatment models.Intensive Outpatient Program or IOP
IOP offers serious clinical support with more flexibility. Verified guidance describes IOP as involving several hours a day, multiple days a week, in common structures, with some programs running more frequently depending on need.Standard outpatient care
This is the least intensive level. It frequently includes individual therapy, medication management, recovery check-ins, or group counseling on a more limited weekly schedule.
Why these distinctions matter
Many people talk about “outpatient” as if it were one thing. It is not.
PHP can feel structured and clinically focused. IOP can support someone who is returning to work, school, or family obligations while still receiving multiple therapy sessions each week. Standard outpatient is frequently best for maintenance, ongoing counseling, or later-stage recovery support.
A useful way to think about it is this:
- Inpatient removes the person from daily life.
- PHP recreates much of that structure without overnight stay.
- IOP adds flexibility while preserving meaningful accountability.
- Standard outpatient supports longer-term maintenance.
That progression is one reason outpatient treatment has become so central in real-world care. It creates options for people who need help but also need to keep living their lives.
A Detailed Comparison of Inpatient vs Outpatient Treatment
The difference between inpatient and outpatient becomes much clearer when looked at side by side. The practical question is not just where treatment happens. The practical question is how the person’s day, risk level, support system, and responsibilities line up with the care model.
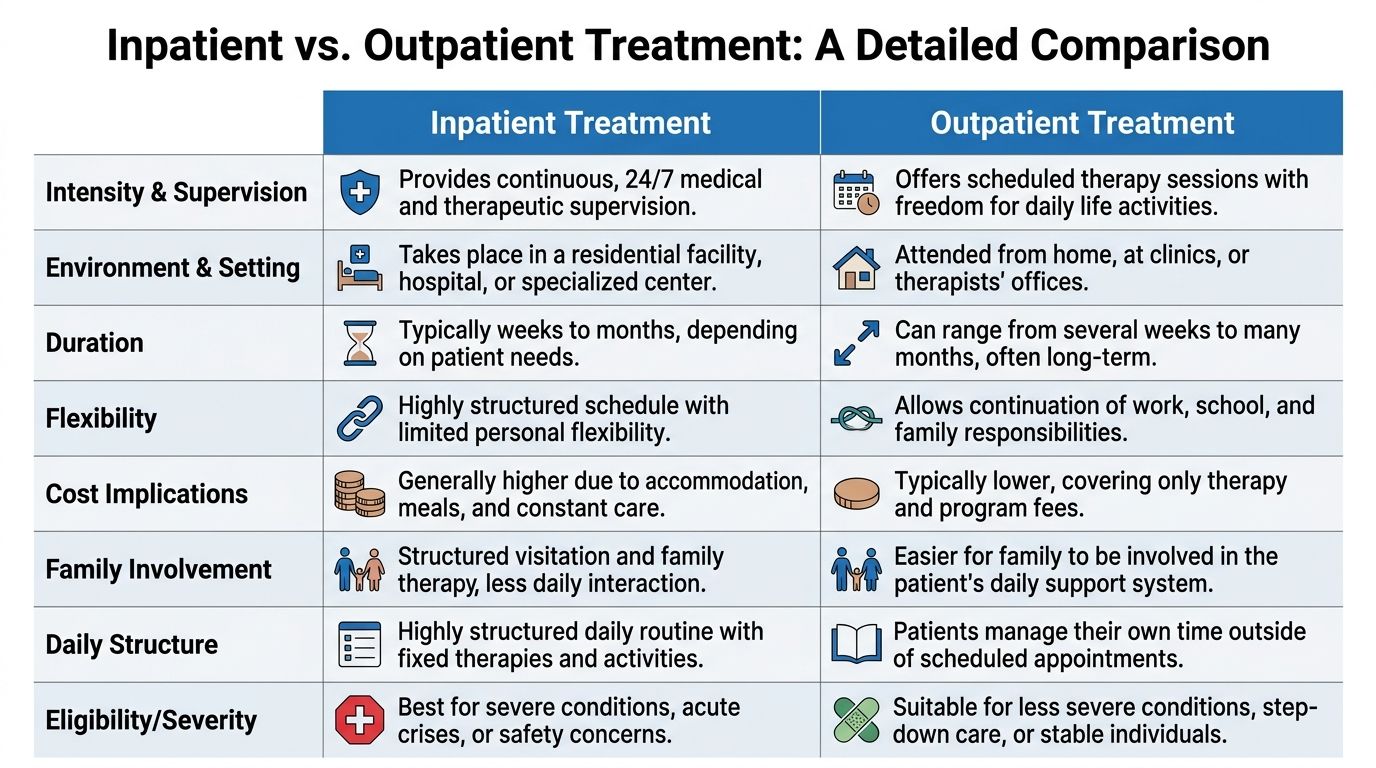
Inpatient vs outpatient care at a glance
| Feature | Inpatient (Residential) | PHP (Partial Hospitalization) | IOP (Intensive Outpatient) |
|---|---|---|---|
| Living arrangement | Lives at the facility | Lives at home | Lives at home |
| Supervision | Continuous supervision | High clinical structure during treatment hours | Structured support during scheduled sessions |
| Best fit | Severe addiction, unstable environment, acute safety concerns | Step-down from inpatient or need for strong support without overnight stay | Stable enough for community living with ongoing therapy needs |
| Daily schedule | Facility controls most of the day | Treatment takes up much of the day | Treatment fits around work, school, or family needs |
| Exposure to triggers | Reduced because environment is controlled | Moderate, since person returns home after sessions | Higher, since person remains in normal routine |
| Family contact | More limited and structured | Easier to involve family | Usually easiest for regular family participation |
| Cost pattern | Generally highest | Usually lower than inpatient | Usually lower than inpatient and often more manageable over time |
A fuller overview of the outpatient continuum appears in this page on outpatient rehab.
The biggest daily difference is clear. Inpatient controls the environment. Outpatient asks the person to practice recovery inside the environment they live in.
Treatment environment
Inpatient care creates separation. That separation can save lives when the home setting is chaotic, unsafe, or full of immediate triggers.
A person who keeps using with friends every night, lives with an abusive partner, or cannot get through a day without spiraling may need that physical reset. Residential treatment builds a temporary container around recovery.
Outpatient care does the opposite. It keeps the person in their real world.
That is not a weakness when the person has enough stability to use it well. In fact, it can be a strength. The person attends treatment, goes home, faces ordinary stress, and then processes what happened in the next session. That loop helps turn therapy into usable habits rather than something learned in isolation.
Intensity and frequency of care
At this point, the difference between inpatient and outpatient becomes most concrete.
Verified clinical guidance states that inpatient programs provide continuous supervision and substantial daily therapy, while standard outpatient care may involve less frequent therapy per week. That distinction is summarized in this overview of inpatient vs outpatient intensity and structure.
PHP and IOP sit in the middle. They are not casual care.
PHP often functions as a high-accountability level for people who need frequent therapy, psychiatric support, and routine. IOP is less immersive, but still structured enough to matter. Someone might attend several times a week, participate in group therapy, meet individually with a clinician, and continue medication support if needed.
A short example makes the contrast easier to see:
- Inpatient might fit someone who cannot stop using for even one day outside a controlled setting.
- PHP might fit someone leaving detox who is medically stable but still fragile.
- IOP might fit someone who can remain sober between sessions with support, accountability, and transportation.
- Standard outpatient might fit someone with early stability who mainly needs ongoing therapy and relapse prevention work.
Program duration
Inpatient treatment is shorter and more concentrated. It is built for stabilization.
Outpatient treatment frequently lasts longer because it supports integration into normal life. That is not a flaw. It is how sustained recovery gets built.
A person may spend time in a residential setting, then move into PHP, then IOP, then standard outpatient or aftercare. Another person may start in IOP and never need inpatient at all. The timeline depends on the person’s symptoms, home life, substance history, and progress in care.
Level of client autonomy
Inpatient care sharply limits autonomy for a reason. The person is in treatment full time. Wake-up times, meals, groups, medication schedules, and daily activities are tightly managed.
That level of control helps people who are not currently making safe decisions on their own.
Outpatient care gives back more responsibility. The person has to show up on time, avoid substance use between sessions, manage transportation, handle conflict at home, and use coping skills outside the therapy room.
That freedom is either therapeutic or dangerous. It depends on the person.
A working adult in Dallas with a supportive spouse and a stable job may benefit from keeping that autonomy. A person who disappears for days, cannot maintain medication, or repeatedly leaves treatment early may need more structure than outpatient can provide at the start.
Approach to family involvement
Family involvement tends to look different across levels of care.
In inpatient treatment, family contact is often more structured. That can be useful when boundaries are poor or relationships are inflamed. The program decides how and when involvement helps.
Outpatient care frequently allows more natural family participation. A spouse may notice mood changes quickly. A parent may help with transportation. A partner may join family sessions and practice healthier communication at home that same week.
That immediacy can be powerful.
It also means outpatient is only as strong as the support around it. If family members are actively using, minimizing the problem, or creating chaos, the outpatient model gets much harder to sustain.
Matching the Treatment Level to Your Needs
Choosing the right level of care should be blunt, not vague. If the person is unsafe, unstable, or medically complicated, inpatient should be the first serious consideration. If the person is stable enough to participate consistently while living at home, outpatient may be the smarter fit.

When inpatient is the safer call
Some situations should not be softened.
Inpatient care often makes more sense when any of the following are true:
- Withdrawal may be dangerous: Alcohol, benzodiazepines, and some other substances can create serious withdrawal complications that need close monitoring.
- The home environment is actively triggering: If people in the home are using substances, enabling, threatening, or constantly escalating conflict, outpatient care starts with a disadvantage.
- There have been repeated relapses after lower levels of care: More freedom is not always the answer. Sometimes the answer is more containment.
- Co-occurring mental health symptoms are severe: Suicidal thinking, psychosis, extreme instability, or inability to function day to day often require a higher level of support.
- The person cannot maintain basic accountability: Missed appointments, disappearing, refusing medication, or using immediately after prior sessions are strong signs that outpatient may not hold.
If daily life is the thing repeatedly knocking recovery off course, treatment should change the daily environment first.
When outpatient is a strong fit
Outpatient should not be treated like a lesser version of care. For the right person, it can be the most practical and effective option.
Verified evidence notes that for people with stable home support, outpatient programs such as IOP and PHP can significantly reduce long-term relapse risk compared to inpatient care in some follow-up studies, because patients start practicing coping skills in real-world settings from day one. That finding appears in this NCBI overview of treatment settings and effectiveness.
Outpatient is frequently a strong fit when:
- The person has stable housing: Recovery is easier when there is a safe place to sleep and a predictable routine.
- Support at home is real, not just promised: Someone needs to be willing to reinforce treatment, not sabotage it.
- Work, school, or parenting responsibilities matter: Many adults cannot realistically leave life behind. Outpatient allows treatment without total disruption.
- The person is motivated and able to attend consistently: Motivation does not need to be perfect, but it does need to be workable.
- Step-down care is needed after inpatient: This is one of the best uses of PHP and IOP.
A more focused explanation of this level appears in this article on what IOP therapy is.
A practical self-check
A family trying to decide between inpatient and outpatient can ask five direct questions:
- Can the person stay physically safe at home right now?
- Can they make it to treatment consistently without disappearing or using first?
- Does home support recovery, or destroy it?
- Have lower levels of care already failed because the structure was too loose?
- Does real life practice help this person, or overwhelm them?
If the answers point toward instability, inpatient is often the cleaner and safer decision.
If the answers point toward stability with meaningful support, outpatient deserves serious consideration. It frequently gives people a better chance to build recovery where they live.
Understanding Costs and Insurance Coverage in Texas
Cost keeps many families stuck. They delay the call, assume treatment will be unaffordable, or pick a level of care based only on fear of the bill.
That often leads to bad decisions.

Why outpatient often feels more manageable financially
In Texas, insurance frequently makes outpatient treatment easier to sustain over time. Verified guidance notes that many PPO plans cover a significant portion of outpatient IOP/PHP sessions compared with a somewhat lesser portion of inpatient days after the deductible is met. That overview appears in this article about how to tell if outpatient or inpatient care is needed.
That does not mean outpatient is always cheaper in every case. Plans vary. Deductibles vary. Networks vary. Preauthorization rules vary.
It does mean families should not assume inpatient is the only serious option. For many people in Dallas-Fort Worth, outpatient may be both clinically appropriate and financially more realistic.
A related question comes up frequently. Will insurance help with addiction treatment at all?
In many cases, yes. The smarter move is to verify benefits early instead of guessing. This resource on whether outpatient rehab services are covered by insurance outlines the kinds of coverage questions families often need answered.
What families in DFW should ask before starting care
Insurance conversations go better when the family asks direct questions.
- Ask about the exact level of care: Coverage for PHP can look different from coverage for IOP or standard outpatient.
- Check whether preauthorization is required: Delays often happen here, especially when nobody asks up front.
- Confirm in-network status: Out-of-network care can change the financial picture quickly.
- Request expected patient responsibility in writing: Families should know whether they are dealing with copays, coinsurance, deductibles, or a combination.
- Ask how continued stay reviews work: Approval for treatment is often tied to ongoing clinical review.
The worst time to figure out insurance is after admission, when stress is high and the family feels cornered.
For people in Euless, Dallas, and surrounding communities, the simplest path is usually to verify benefits early instead of guessing. That turns the cost conversation from a guessing game into a decision with real numbers attached.
How to Transition Between Levels of Care
Recovery rarely moves in one straight line. A person may need detox first, then a more structured setting, then a gradual return to normal life. Another person may start in outpatient and step up temporarily if symptoms worsen.
That movement is normal.

Step-down care is progress
Many people hear “step-down” and assume it means treatment is becoming less serious. That is the wrong way to think about it.
Stepping down usually means the person has gained enough stability to handle more responsibility. They do not need the same amount of containment.
A common path looks like this:
- Detox for withdrawal stabilization when needed
- Residential or inpatient treatment for intensive support
- PHP for structured daytime care without overnight stay
- IOP for continued therapy while returning to daily responsibilities
- Standard outpatient or aftercare for ongoing support and relapse prevention
Each level has a job. The sequence helps the person carry treatment gains into ordinary life instead of losing momentum after discharge.
What a smooth transition looks like
A solid transition is not just a discharge date. It includes practical planning.
The treatment team should identify current triggers, medication needs, transportation issues, therapy schedule, family involvement, and what happens if cravings spike. If the next level is outpatient, the first appointments should be arranged quickly so there is no empty stretch between programs.
Good transitions usually include:
- Clear handoff communication: The next provider should know what the person was working on and what still needs attention.
- Medication continuity: Gaps in psychiatric medication or MAT can destabilize progress quickly.
- Family expectations: Loved ones need to understand what support helps and what behavior enables.
- Relapse response planning: If the person slips, everyone should know the next step instead of reacting with chaos.
A strong continuum of care turns treatment from an isolated event into an actual recovery process.
During this phase, many people either build traction or lose it. The transition phase deserves as much attention as the initial admission decision.
Take the First Step Toward Recovery in Euless and Dallas
The difference between inpatient and outpatient is not complicated once the focus stays where it belongs. Inpatient is for higher risk, tighter structure, and stronger environmental control. Outpatient is for treatment that works inside real life.
Neither is automatically better.
The better option is the one that matches the person’s current stability, medical risk, mental health needs, family environment, and ability to follow through. If home is unsafe or withdrawal is dangerous, inpatient is frequently the right answer. If the person has support, housing, accountability, and a real reason to stay engaged in daily life, outpatient can be a strong and practical path.
That matters in Euless and across the Dallas-Fort Worth area, where many adults are trying to get help without losing work, school progress, parenting responsibilities, or connection to family. Those realities should not be ignored. They should be built into the treatment decision.
A family does not need to settle this alone. A proper clinical assessment can sort out whether someone needs detox, residential treatment, PHP, IOP, standard outpatient care, or a step-down plan that combines levels over time.
Waiting often makes the decision harder. Symptoms deepen. Trust erodes. Logistics get worse.
The next step should be simple. Get an honest assessment, ask direct insurance questions, and choose the level of care that gives the person the best chance to stay engaged long enough for treatment to work.
Maverick Behavioral Health helps adults in Euless, Dallas, and the surrounding DFW area find the right outpatient path for substance use and co-occurring mental health treatment. Programs include PHP, IOP, standard outpatient care, dual diagnosis support, and MAT including Suboxone for opioid dependence. To speak with a compassionate admissions team member and schedule a free, confidential assessment, call (888) 385-2051 or visit Maverick Behavioral Health.