

A lot of people in Dallas-Fort Worth don’t start out trying to develop an addiction. They start by trying to get through the day.
A drink after work takes the edge off. A pill makes sleep possible. Marijuana quiets racing thoughts for a few hours. Stimulants help someone stay productive when anxiety and exhaustion are already running the show. For a while, the substance looks like a coping skill. Then it starts creating new problems, and the original stress, sadness, trauma, or loneliness is still there.
That’s where coping skills addiction becomes an important conversation. The issue isn’t only the substance itself. The issue is that the brain and body learned to treat that substance as the main answer to discomfort. Recovery gets stronger when a person replaces that one harmful answer with a personalized set of healthier responses that fit real life.
Table of Contents
- Why Healthy Coping Skills Are Important for Addiction Recovery
- Identifying Your Personal Addiction Triggers
- Building Your Evidence-Based Coping Skill Toolkit
- How to Personalize Your Coping Strategy for Your Unique Needs
- Integrating Coping Skills with Professional Outpatient Treatment
- Creating a Proactive Relapse Prevention Plan
- Frequently Asked Questions About Coping Skills and Recovery
Why Healthy Coping Skills Are Important for Addiction Recovery
A common pattern looks like this. Someone feels stressed, ashamed, lonely, or physically restless. They use a substance and feel relief almost immediately. The brain records that relief and starts treating the behavior like a survival tool.
That short-term payoff is why addiction can feel so confusing. The substance may work for a moment. It may numb grief, reduce social fear, soften trauma symptoms, or shut off intrusive thoughts. But the cost keeps rising. Sleep gets worse, relationships become strained, work suffers, and emotional tolerance shrinks.
A person then needs the substance not only for the original pain, but also for the damage caused by using it.
Relief isn’t the same as recovery
Healthy coping skills do something different. They may not create instant escape, but they help a person stay steady enough to move through stress without making life smaller. They build capacity instead of dependency.
A 2023 survey on unhealthy coping and mental health struggles found that 77% of Americans report using unhealthy behaviors to cope with mental health struggles, and 94% agreed that addictions often mask underlying mental health issues. Those numbers fit what clinicians see every day. Substance use often sits on top of untreated pain.
Practical rule: If a behavior brings relief now but consistently creates more chaos later, it isn’t a coping skill. It’s a problem disguised as relief.
Recovery requires replacement, not just removal
People often try to stop using without changing how they respond to pressure. That usually leaves a dangerous gap.
A better approach is to build alternatives for the moments that used to lead straight to use:
- Stress after work: replace automatic drinking or drug use with a transition routine.
- Loneliness at night: replace isolation with planned contact or structured activity.
- Panic or agitation: replace impulsive use with grounding and body-calming skills.
- Numbness or depression: replace shutdown with small, scheduled actions.
This is why coping skills addiction work matters so much. Sobriety isn’t only about resisting a substance. It’s about learning how to handle anger, boredom, grief, cravings, conflict, and empty time without reaching for the old solution.
People don’t need perfect emotional control. They need skills they can use on a hard Tuesday in traffic, after an argument, during a lonely weekend, or when cravings hit at 10 p.m.
Identifying Your Personal Addiction Triggers
Most relapses don’t come out of nowhere. They usually build from a sequence. A feeling shows up. A thought follows. Then a behavior starts pulling the person toward the old pattern.
That’s why trigger work has to get specific. “Stress” is too vague to help much. It’s more useful to know that cravings spike after criticism from a supervisor, during the drive past a familiar liquor store, after getting paid, or when an ex sends a late-night text.

Recovery gets more stable when a person can spot those patterns early. Data on addiction recovery and relapse notes that relapse rates for substance use disorders are between 40-60%, but drop to less than 15% after 5 years of sustained recovery. One reason long-term recovery becomes more stable is that people get better at recognizing triggers before those triggers turn into action.
Start with a simple trigger map
A useful exercise is to review one ordinary day from morning to night. The goal isn’t to write a life story. The goal is to find repeating pressure points.
Ask these questions in writing:
- When did discomfort start? Note the time and what was happening.
- What was felt first? Anxiety, anger, boredom, shame, sadness, emptiness, tension.
- What thought came next? “I need a break.” “I can’t handle this.” “One time won’t matter.”
- What urge followed? Drink, use, text a dealer, isolate, stop eating, skip a meeting.
- What would have helped in that exact moment? Leaving, calling someone, eating, breathing, walking, delaying.
This exercise often reveals that use isn’t random. It’s linked to predictable moments.
Common trigger categories include:
- People: certain friends, family conflict, romantic stress, social pressure.
- Places: bars, neighborhoods, parked cars, bathrooms at work, specific routes home.
- States: hunger, anger, fatigue, panic, shame, physical pain, overstimulation.
- Situations: payday, weekends, being alone, celebrations, conflict, downtime.
Use HALT before a craving gets louder
HALT is simple because it works. It reminds a person to check four states that often lower judgment and increase vulnerability.
- Hungry: Low blood sugar and skipped meals can make irritability and urges worse.
- Angry: Unexpressed anger often pushes people toward fast relief.
- Lonely: Isolation amplifies cravings because no one is there to interrupt the spiral.
- Tired: Exhaustion weakens follow-through and makes old habits feel easier.
Cravings often sound psychological, but many start with a body that’s depleted, a mind that’s overloaded, or a nervous system that hasn’t had a chance to settle.
HALT isn’t the whole plan. It’s an early warning screen. If someone checks in and realizes they’re hungry, furious, disconnected, and exhausted, that moment needs care right away. Not later.
A practical routine is to do a HALT check at the same times every day. Midday. End of work. Before bed. That kind of repetition helps cravings feel less mysterious and more manageable.
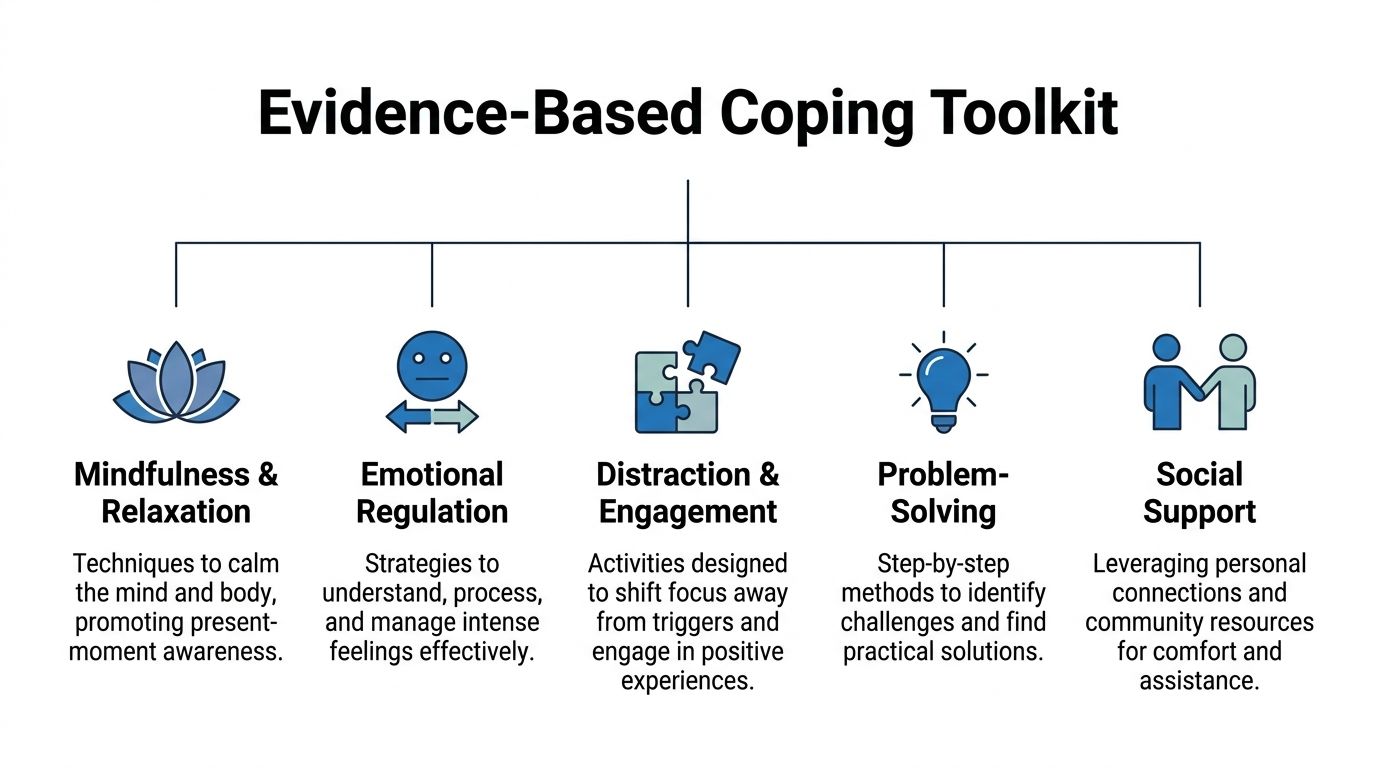
Building Your Evidence-Based Coping Skill Toolkit
People in recovery often hear advice like “journal,” “take a walk,” or “call someone.” Sometimes that helps. Sometimes it doesn’t. A key issue is whether the skill matches the job that needs to be done.
A strong toolkit covers different kinds of distress. Some skills work on thoughts. Some lower emotional intensity. Some calm the body. Others interrupt isolation and shame. The best plan includes several types, because no single technique works for every trigger.
One evidence-based foundation is CBT. CBT outcomes in addiction treatment reports effectiveness up to 60% for alcohol addiction, and notes that people who remain in treatment for 90 days or more have significantly better long-term outcomes. That matters because coping skills improve with repetition. A person usually doesn’t think their way out of a craving once and become set for life. Skills need practice until they become usable under pressure.
Cognitive skills that change the thought pattern
These tools target the internal story that fuels using.
Thought stopping.
When the brain starts repeating permission-giving thoughts, the person labels the pattern clearly. “That’s craving talk.” Then they interrupt it with a planned replacement statement such as, “Using will make tonight harder, not easier.”
Check the consequence.
A craving usually highlights the first ten minutes and hides the next two days. This exercise asks one question: “What happens next if this goes forward?” It pulls the brain out of fantasy and back into cause and effect.
Urge delay.
Instead of arguing with the urge forever, the person delays action for a set period and does one alternate behavior first. Even a short delay can weaken the sense of urgency.
Emotional skills that lower the intensity
Some people don’t need to analyze more. They need to survive the feeling without acting on it.
Name the feeling accurately.
“I feel bad” is too broad. “I feel rejected and embarrassed” is more useful. Specific language often lowers intensity because it turns chaos into something more workable.
Ride the wave.
Urges rise, peak, and fall. A person notices the craving like a wave instead of treating it like a command. The task is to observe it, breathe through it, and let it pass without feeding it.
Self-soothing with intention.
This isn’t mindless escape. It’s deliberate calming through music, a shower, a blanket, tea, prayer, or quiet sensory input that reduces overwhelm without creating more damage.
Somatic skills that calm the body fast
A lot of cravings are body-first experiences. The chest tightens. The jaw clenches. The legs feel restless. Thinking clearly is hard when the nervous system is already activated.
4-7-8 breathing.
Inhale through the nose for 4, hold for 7, exhale for 8. Repeating the cycle can slow the stress response and create enough space to make a better decision.
Grounding through the senses.
Look for five things in sight, four that can be touched, three that can be heard, two that can be smelled, and one that can be tasted. This works especially well when panic or dissociation is part of the trigger.
Movement that changes state.
A brisk walk, stretching, bodyweight exercises, or mindful movement can discharge tension. Gentle mind-body practices can also support regulation, and some people benefit from exploring approaches like qi gong and yoga in recovery.
A coping skill doesn’t have to feel profound to be effective. If it lowers activation enough to prevent a bad decision, it did its job.
Social skills that interrupt isolation
Addiction grows well in secrecy. Recovery usually doesn’t.
Use a script before there’s a crisis.
Many people don’t call for help because they don’t know what to say. A short script helps: “I’m having a rough craving and need ten minutes on the phone.”
Build a contact ladder.
One person may not always answer. A better plan includes several levels of support, from a close friend to a therapist to a meeting or recovery group.
Practice honest check-ins.
The goal isn’t sounding polished. It’s saying what’s true before the situation gets worse.
Your Quick-Reference Coping Skills Menu
| Skill Category | What It Does | Example Exercise |
|---|---|---|
| Cognitive | Interrupts thoughts that justify use | Write the craving thought, then write a more accurate replacement |
| Emotional | Helps tolerate feelings without acting impulsively | Set a timer and ride the urge while naming the emotion precisely |
| Somatic | Reduces physical activation and stress response | Practice 4-7-8 breathing for several rounds |
| Social | Breaks secrecy and brings in accountability | Text or call a trusted support person with a clear script |
| Behavioral | Replaces using with a healthier action | Leave the triggering place and take a structured walk |
A toolkit should stay visible. Keep it in a phone note, wallet card, journal, or taped inside a cabinet door. When stress hits, memory gets worse. The plan should be easy to find.
How to Personalize Your Coping Strategy for Your Unique Needs
Generic recovery advice often falls apart because different people use substances for different reasons. Someone who drinks to numb social anxiety needs a different first-line response than someone who uses stimulants to push through depression and exhaustion.
That’s why one-size-fits-all lists can become frustrating. The skill may be “good,” but still be wrong for the person.

A clinical discussion of coping skills therapy and personalization points to a major gap in recovery guidance. Plans work better when they align with a person’s neurobiology, trauma triggers, and mental health comorbidities. In practice, that means matching the intervention to the pattern instead of forcing the same answer onto every client.
Match the skill to the pattern
A personalized plan usually starts with three questions.
What substance has been doing the job?
Alcohol and sedatives often serve as shutdown tools. Stimulants often serve as activation tools. Opioids may blunt emotional and physical pain. The substitute skill should address the same pressure point in a safer way.
What mental health symptoms are involved?
Someone with anxiety may need grounding, breathwork, and exposure to avoided situations. Someone with depression may need behavioral activation, structured routine, light movement, and accountability. Someone with trauma may need stabilization before deeper emotional processing.
What happens under stress?
Some people isolate. Others become impulsive. Others freeze and stop functioning. Their coping toolkit should fit that pattern.
A few examples make this clearer:
- If panic drives the urge to drink, fast body-calming tools may work better than long journaling sessions.
- If depression leads to lying in bed and then using, activation matters more than meditation alone.
- If shame follows conflict and triggers relapse, a repair script and support call may be more useful than trying to “think positive.”
- If boredom fuels use, passive distractions may not be enough. The person may need scheduled structure and meaningful activity.
What often doesn’t work
Some strategies fail not because the person is weak, but because the fit is poor.
- Overcomplicated plans: A ten-step routine won’t help during an intense craving if it’s too hard to remember.
- Skills that depend on high motivation: When a person is depleted, they need low-friction tools.
- Advice that ignores trauma: Some mindfulness practices can feel overwhelming for trauma survivors if they increase internal exposure too quickly.
- Shame-based self-talk: Harsh inner criticism usually increases risk. It rarely builds stability.
The right question isn’t “What coping skill is best?” It’s “What coping skill is most likely to work for this person in this situation?”
This is one area where individualized outpatient treatment can help. In Euless and the broader Dallas area, clinicians may look at timing, symptoms, substance history, environmental triggers, and daily routine to help a person build a toolkit they’ll use.
Integrating Coping Skills with Professional Outpatient Treatment
Self-help strategies matter. They can reduce harm immediately and help a person gain traction. But many people need more than a list on their phone. They need structure, feedback, and repetition in a setting where the work keeps moving even when motivation drops.
That’s where outpatient treatment often changes the picture. A person can keep living at home, keep working or handling family responsibilities, and still get regular support focused on real-world triggers.
Why structure matters
Coping skills sound simple in theory. The hard part is using them at the exact moment old habits start pulling. Professional treatment gives that learning process more support.
Individual therapy can help uncover the actual function of substance use. Group therapy gives people a place to practice honesty, boundaries, and communication instead of staying trapped in secrecy. A higher level of outpatient care can also create accountability across the week, not just once in a while.
For people who need a clearer framework, this overview of what IOP therapy is and how it works explains how structured outpatient care fits into recovery.
Where outpatient care helps most
Professional support tends to help in a few key areas:
- Assessment: Clinicians can identify whether cravings are being driven by trauma, depression, anxiety, withdrawal, routines, or social pressure.
- Customization: Skills can be matched to actual triggers instead of copied from a generic checklist.
- Practice: Repetition happens in therapy, groups, and daily assignments until the responses become more natural.
- Adjustment: If a skill isn’t working, the plan can change instead of leaving the person stuck.
- Medication support: For opioid or alcohol use in particular, medication-assisted treatment can reduce cravings enough for learning and behavior change to take hold.
In the Dallas-Fort Worth area, some people need standard outpatient support. Others need the added intensity of PHP or IOP for a period of time. Some also need dual diagnosis treatment because untreated mental health symptoms keep pulling them back toward use. Maverick Behavioral Health provides outpatient substance use and mental health treatment in Euless, including IOP, PHP, standard outpatient care, dual diagnosis services, group and individual therapy, and MAT including Suboxone.
Professional care doesn’t replace personal responsibility. It gives that responsibility a better chance to succeed.
Someone who’s trying to stop using while also dealing with cravings, anxiety, poor sleep, relationship strain, and a full work schedule isn’t failing because they need help. They’re dealing with a complicated problem that usually responds better to skilled support.
For a confidential conversation about treatment options in Euless or the Dallas area, call (888) 385-2051.
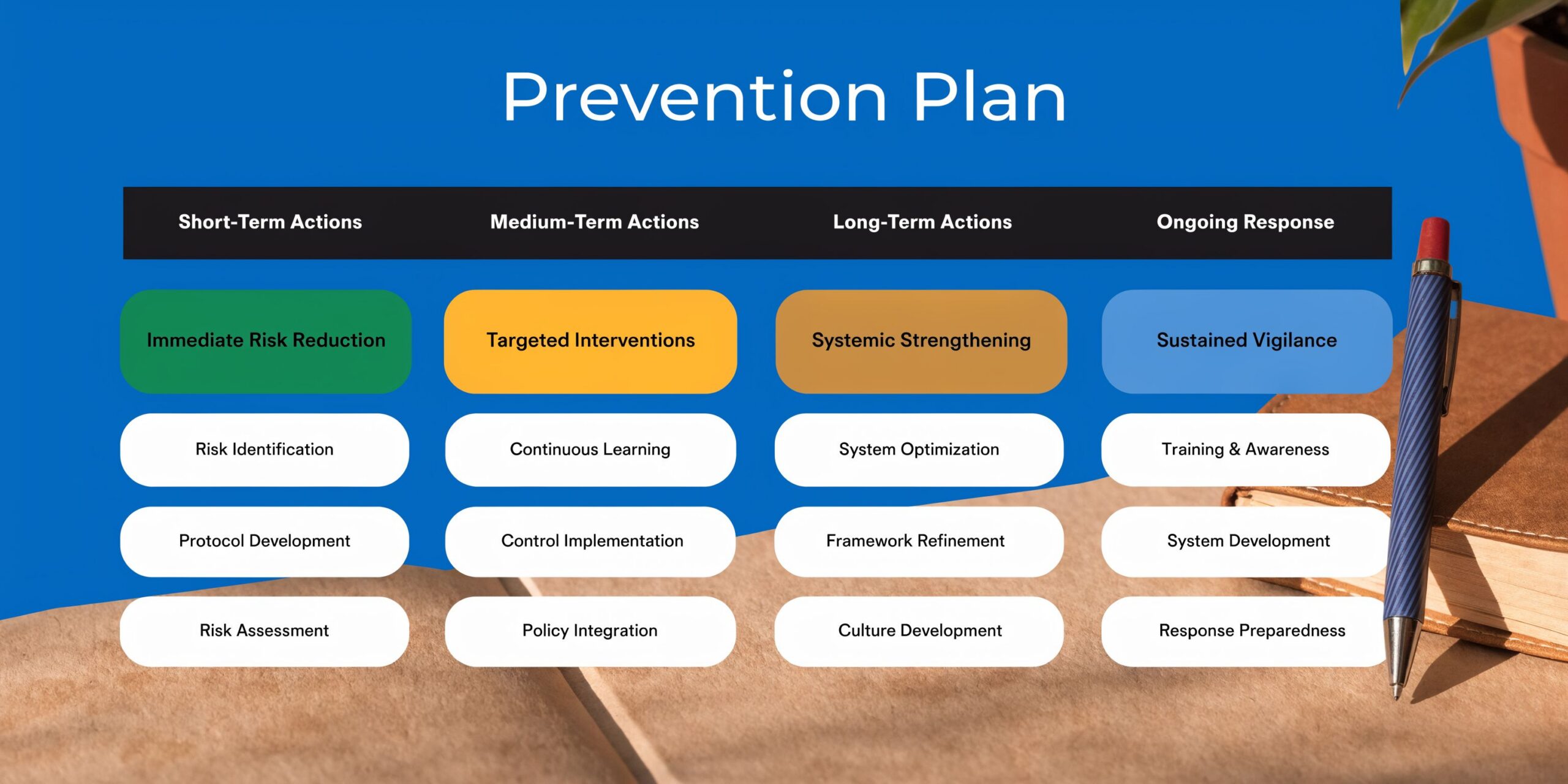
Creating a Proactive Relapse Prevention Plan
A relapse prevention plan should be written down. Not held vaguely in memory. Not based on hoping the next craving won’t be too strong.
When stress rises, decision-making gets narrow. A written plan gives the brain something concrete to follow before panic, secrecy, or impulse takes over.
A useful plan is short enough to use and specific enough to matter. For more practical guidance, this article on relapse prevention strategies for staying sober after rehab in Dallas can help people think through the details.
What to put in writing
A solid relapse prevention plan usually includes these pieces:
High-risk situations
Write down the moments most likely to trigger use. Be concrete. “After fights with partner,” “driving home from work,” “being alone on payday,” “Sunday evenings.”A response for each trigger
Match every risk with an action. If the trigger is late-night loneliness, the response might be a support call, a meeting, or leaving the house for a safe activity. If the trigger is panic, the response might be breathing, grounding, and contacting a therapist.Support contacts
List at least three people or supports in order. Include phone numbers. Don’t rely on memory.Daily stabilizers
Put the basics on the plan. Meals, sleep routine, medication adherence if prescribed, movement, transportation, and scheduled support.
What to do after a lapse
A lapse needs a response, not a collapse.
Many people make things worse by turning one use episode into a full return to the old pattern. Shame tells them they’ve already ruined everything, so they might as well keep going. That’s exactly when the written plan matters most.
Include a post-lapse section such as:
- Tell someone quickly: Don’t hide it.
- Leave the risky environment: Create immediate distance from access and triggers.
- Return to treatment or support: Reconnect fast instead of waiting for things to get worse.
- Review what happened: Identify the point where the plan broke down.
- Restart the routine: The next healthy action matters.
A lapse is a signal that the plan needs strengthening. It isn’t proof that recovery is over.
It also helps to include reasons for staying sober that are personal and specific. Children. Health. Sleep. Career stability. Repairing trust. Self-respect. A future that feels possible. Those reminders can matter when cravings try to reduce life to one moment.
Frequently Asked Questions About Coping Skills and Recovery
People usually don’t struggle because they’ve never heard of coping skills. They struggle because applying them in real life is harder than reading about them. A few practical questions come up often.
| Question | Answer |
|---|---|
| How many coping skills should a person have? | More than one. A small toolkit is stronger than a single favorite strategy because different triggers need different responses. |
| What if a coping skill doesn’t work right away? | That doesn’t always mean the skill is wrong. It may need more practice, better timing, or a better fit for the specific trigger. |
| Are coping skills enough without treatment? | Sometimes they help a person stabilize. But if cravings, relapse risk, mental health symptoms, or daily functioning are getting worse, professional support is often the safer move. |
| What’s the best first coping skill during a craving? | The best first step is usually the one that creates immediate interruption. Leave the triggering place, contact support, or calm the body fast. |
| Can coping skills help with both addiction and mental health symptoms? | Yes. Many of the same skills support both, especially when anxiety, depression, trauma, or stress are tied to substance use. |
Common concerns that deserve direct answers
Some people worry that needing coping skills means they should be able to “handle it on their own” by now. That belief keeps a lot of people stuck. Recovery is a skill-building process, not a character test.
Others assume healthy coping should feel as powerful as the substance did. Usually it doesn’t. Healthy skills often feel quieter at first. But they build stability instead of debt.
Another common concern is boredom. Life in early recovery can feel flat because the nervous system is adjusting. That doesn’t mean recovery isn’t working. It usually means the person needs more structure, connection, and meaningful routine while the brain and body settle.
The most important takeaway is simple. Coping skills addiction work isn’t about finding one perfect trick. It’s about building a repeatable system that fits the person, the trigger, and the stage of recovery.
People in Euless, Dallas, and the surrounding DFW area don’t have to figure this out alone. Maverick Behavioral Health helps adults build practical coping tools for addiction and co-occurring mental health needs through outpatient care, including IOP, PHP, standard outpatient treatment, and MAT support. To talk through options confidentially, call (888) 385-2051.