


Some people in Dallas, Euless, and the wider DFW area are reading this after months of telling themselves the same thing: the drinking, pills, cannabis, cocaine, or other substance use is just a phase, and the sadness, numbness, irritability, or exhaustion will pass once life settles down. Families often see the pattern sooner. A person starts missing work, withdrawing from people they love, sleeping at odd hours, or seeming “fine” only when they’re using something.
When both problems are happening at the same time, it can feel confusing. Is the depression causing the substance use, or is the substance use causing the depression? In many cases, the answer is both. That’s why depression and substance abuse treatment works best when both issues are treated together, not one after the other.
This kind of care is often called dual diagnosis treatment. The term sounds technical, but the idea is simple. One treatment plan addresses the emotional pain and the substance use at the same time. For families in DFW, that often means looking for outpatient care that fits real life, including work, school, parenting, transportation, and insurance questions. Help is available, and a first conversation can start by calling (888) 385-2051.
Table of Contents
- When It’s More Than Just One Thing Starting Your Recovery
- The Tangled Link Between Depression and Substance Abuse
- Signs It’s Time to Seek Dual Diagnosis Treatment
- Your Path Forward Evidence-Based Treatment Options
- What Your Recovery Journey Looks Like Day to Day
- Making Treatment Accessible Navigating Insurance and Costs
- Life After Treatment Building Lasting Recovery in DFW
When It’s More Than Just One Thing Starting Your Recovery
A lot of people don’t walk into treatment saying they have a co-occurring disorder. They say they can’t get out of bed without feeling dread. They say they drink at night to quiet their mind. They say they use something just to feel normal enough to get through the day. Families usually describe a loved one who looks overwhelmed, flat, restless, or unlike themselves.
That experience has a name, and naming it can be a relief. Dual diagnosis means a person is dealing with both a mental health condition, such as depression, and a substance use disorder. It isn’t a character flaw or a sign that recovery is less likely. It means treatment has to match what’s really happening.

Why this matters so much
The need for care is large, and many people still go without it. In 2023, nearly 54.2 million people aged 12 and older needed substance abuse treatment, and only part of that group received care. The same data also showed that 71.1% of adolescents with co-occurring depression and substance use disorder received some form of care, which points to the importance of programs that address both conditions together, according to 2023 treatment data from the National Center for Drug Abuse Statistics.
Those numbers matter because they tell families two things. First, this problem is common. Second, getting the right type of help matters more than trying to “just stop” one piece of the problem while the other keeps driving it.
Practical rule: If low mood and substance use keep feeding each other, a single-focus treatment plan usually leaves one trigger untreated.
What recovery can start to look like
For many people in DFW, recovery doesn’t begin with a dramatic turning point. It starts with a phone call, an assessment, and a plan that feels manageable. Outpatient treatment can help a person get structured support while still staying connected to home, work, or school.
A helpful starting mindset is this:
- It doesn’t have to be sorted out alone. Families often spend months trying to decide what the “real” problem is.
- It doesn’t have to wait for everything to fall apart. A person doesn’t need to lose a job, relationship, or semester before getting help.
- It doesn’t have to mean leaving life behind. Many outpatient programs in the Dallas and Euless area are built for people who still need flexibility.
The Tangled Link Between Depression and Substance Abuse
Depression and substance use often act like two tangled cords in the same drawer. Pulling on one moves the other. A person may start using alcohol or drugs to blunt sadness, anxiety, guilt, or emotional numbness. Over time, the substance use can deepen hopelessness, lower motivation, disrupt sleep, strain relationships, and make it harder for the brain and body to stabilize.
That’s why families get confused. At first, the substance can look like a solution. It may help someone feel more relaxed, more social, more energized, or less emotionally shut down. Later, it often becomes part of the problem.
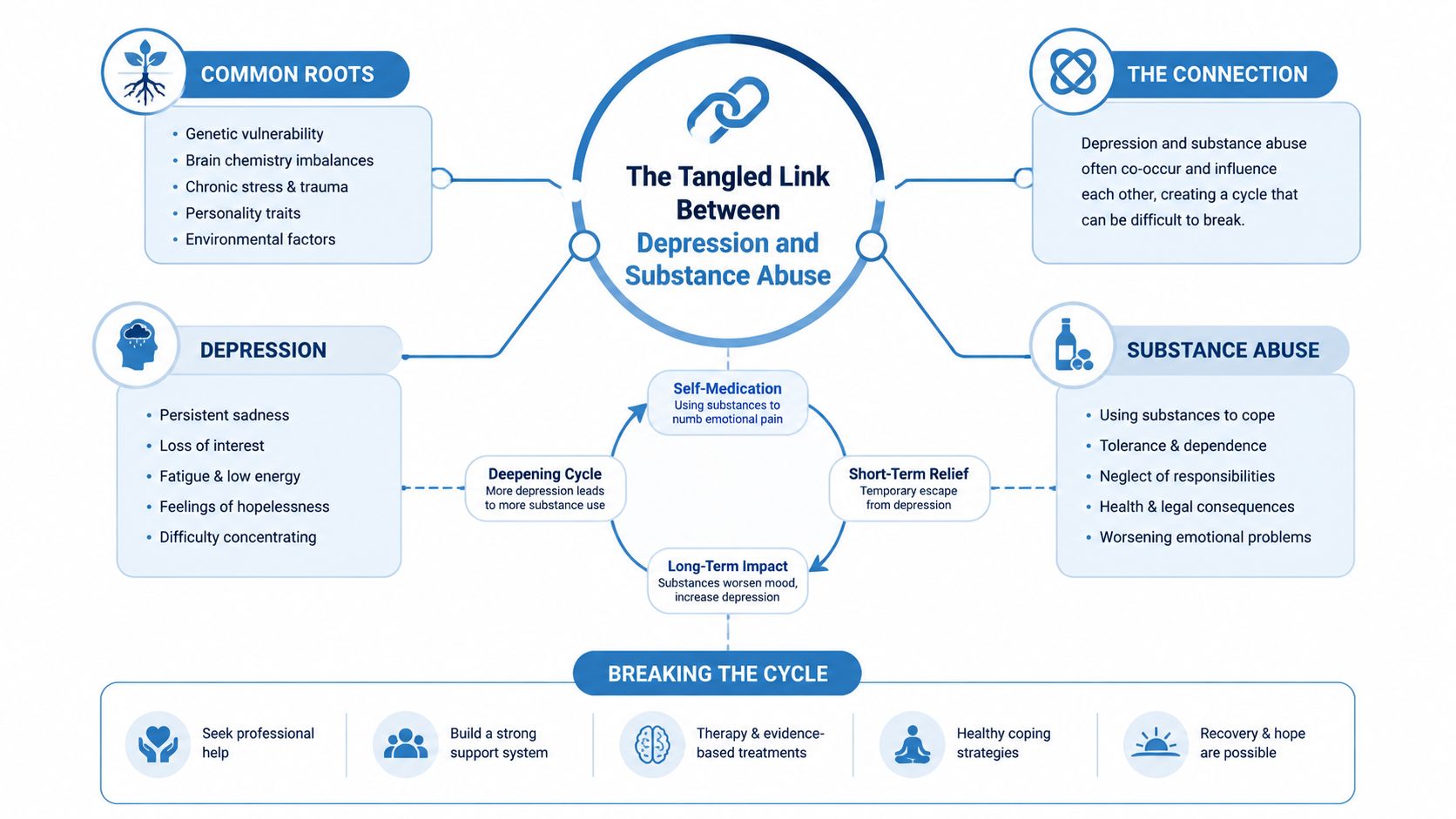
How one problem can fuel the other
A common pattern starts with emotional pain. Someone feels empty, discouraged, ashamed, exhausted, or disconnected. They use a substance for relief. That relief is temporary. Afterward, they may feel more depressed, more physically depleted, and more behind in daily life. Then the urge to use again grows stronger.
Research supports that this relationship runs in both directions. For every 1-point increase in substance use disorder severity, depression scores increased by 0.44 points, and having a substance use disorder independently doubled the odds of developing moderate-to-severe depression, according to longitudinal findings published in the National Library of Medicine.
That kind of finding helps explain why “just treating the addiction” or “just treating the depression” often doesn’t hold. When one side is ignored, the other side can quickly pull the person back into the same cycle.
What this looks like in real life
Families often notice patterns like these:
- Relief that backfires. Someone drinks to sleep, then wakes up more anxious, foggy, and down.
- Motivation that disappears. A person uses a stimulant to push through work, then crashes harder and feels more hopeless afterward.
- Isolation that grows. Substance use starts as private coping and slowly replaces connection, routine, and trust.
Treating only one half of the cycle is like fixing one flat tire and expecting the whole car to drive straight.
Why integrated care matters
Integrated treatment puts both issues on the same care plan. That means the therapist, medical team, and recovery support all work from the same picture. If someone has cravings after a painful family conflict, that isn’t treated as only an addiction issue. If someone feels severe depression after stopping a substance, that isn’t treated as only a mood issue. Both are addressed together.
That approach usually feels less frustrating for the person in treatment and for the family trying to support them. It also gives the treatment team a clearer way to understand setbacks, progress, medication response, and relapse risk.
Signs It’s Time to Seek Dual Diagnosis Treatment
People rarely need help because of one dramatic symptom alone. More often, there’s a cluster of changes that build over time. A family member may seem sad and irritable at once. A spouse may notice drinking has become a daily routine. A student may stop caring about classes, sleep through alarms, and insist nothing is wrong.
When depression and substance use overlap, a gentle self-check can help connect the dots.
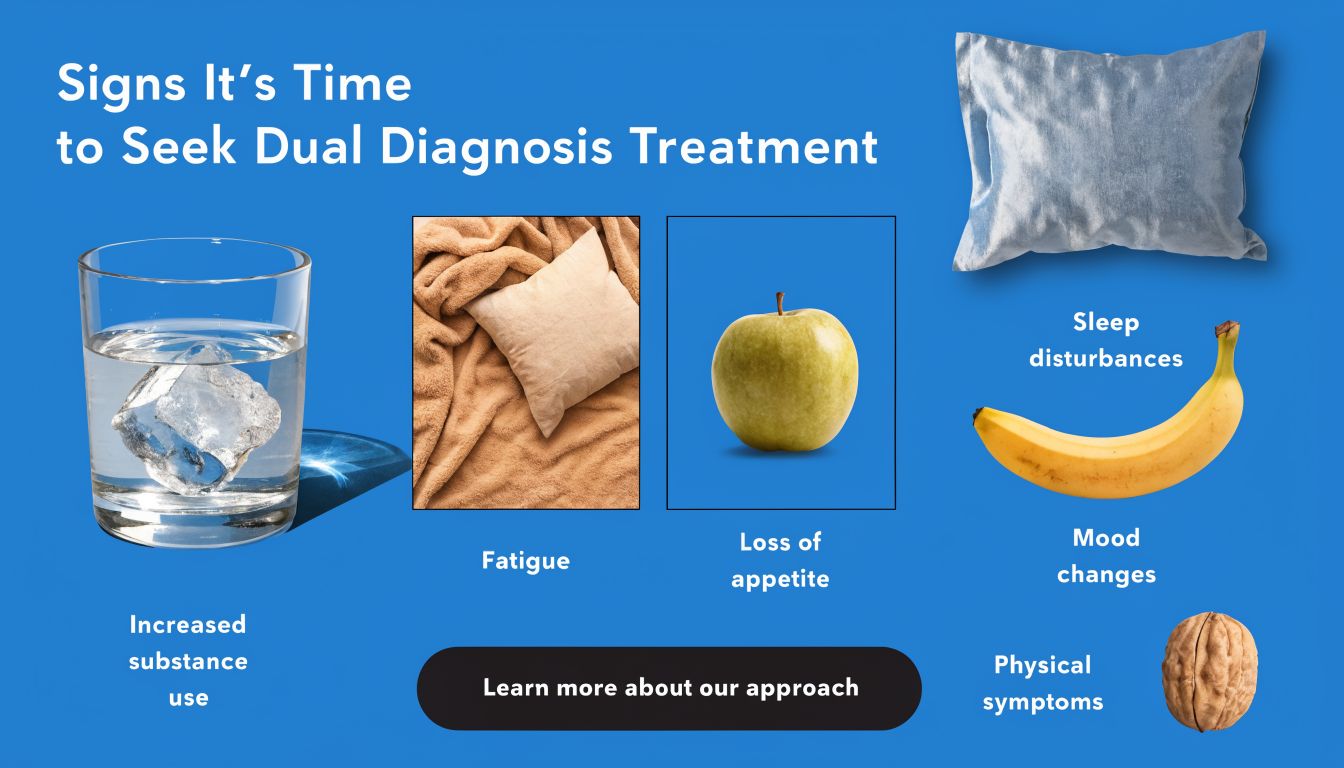
Changes in daily life
Sometimes the clearest warning signs are practical. The person who used to keep up with responsibilities starts falling behind. Calls go unanswered. Meals get skipped. Bills stack up. Hygiene slips. Work performance changes. The person may spend more time alone or only show up socially when substances are involved.
A family may also notice repeated cycles. There’s a promise to cut back, a few better days, then another crash.
Changes in emotional life
Depression doesn’t always look like crying. It can look like anger, numbness, sarcasm, guilt, or no energy for anything. Some people say they feel “flat” unless they’re using. Others describe a constant heaviness they can’t explain.
These emotional signs often deserve attention:
- Persistent hopelessness. The person talks as if nothing will improve.
- Irritability or emotional swings. Small stressors trigger outsized reactions.
- Loss of interest. Activities, relationships, or goals that once mattered no longer seem worth the effort.
Changes in the relationship with substances
Families often ask when use becomes treatment-worthy. A useful answer is this: when the person can’t reliably control it, and life keeps shrinking around it.
Common signs include:
- Using for emotional relief. Substances become the main way to sleep, relax, escape, or feel okay.
- Needing more over time. The old amount no longer feels like enough.
- Trying to stop and not staying stopped. Good intentions keep collapsing under stress, cravings, or depressed mood.
A person doesn’t have to “hit bottom” to qualify for help. If the pattern is repetitive, painful, and hard to interrupt, treatment is worth considering.
For readers who want a fuller look at how co-occurring care works, this overview of dual diagnosis rehab can help clarify what coordinated treatment involves.
Your Path Forward Evidence-Based Treatment Options
A lot of DFW families reach this point feeling stuck between concern and logistics. They can see that depression and substance use are feeding each other, but they still need a practical answer to a basic question. What kind of help fits this person’s life right now?
Outpatient treatment usually works best when it is integrated. In plain terms, the same treatment team addresses mood symptoms, substance use, relapse triggers, therapy goals, and medication needs in one plan. That matters because treating only the depression or only the substance use often leaves the other problem pulling the person backward. Research on co-occurring depression and substance dependence has found better treatment retention when both conditions are addressed together, according to findings on co-occurring depression and substance dependence.
For families, it can help to picture levels of care like different amounts of scaffolding around a house under repair. The house is the same person. The question is how much support is needed to keep things stable while real healing begins.
What integrated outpatient care actually includes
A strong outpatient plan usually combines several forms of help at once. Individual therapy gives the person a private place to work through shame, grief, hopelessness, and patterns that keep the cycle going. Group therapy reduces the loneliness that often fuels both depression and substance use. Medication support may help reduce cravings, ease withdrawal, or treat depression when a prescriber believes it is appropriate.
In the DFW area, one outpatient option is Maverick Behavioral Health in Euless. The program offers PHP, IOP, standard outpatient care, dual diagnosis treatment, and medication-assisted treatment based on the person’s needs, schedule, and clinical picture.
Comparing outpatient levels of care
The right level of care depends on current stability, safety, and how much structure the person can realistically use. It is not a moral ranking. It is closer to matching the right cast to the right injury.
| Level of Care | Time Commitment | Best For |
|---|---|---|
| PHP | Most structured outpatient schedule | People who need strong daytime support, close monitoring, and a high level of therapeutic contact without inpatient admission |
| IOP | Moderate structured weekly schedule | People who need consistent therapy and relapse-prevention work while continuing work, school, or home responsibilities |
| Standard Outpatient | Least intensive schedule | People with more stability who still need ongoing therapy, check-ins, and recovery support |
Here is how that often looks in real life for DFW residents.
- PHP often fits early recovery or a rough stretch. If someone is struggling to get out of bed, using frequently, missing responsibilities, or feeling emotionally unsafe, a more structured daytime schedule can create stability quickly.
- IOP often fits people balancing treatment with real life. Many parents, working adults, and college students use this level because it provides meaningful support while leaving room for jobs, classes, childcare, or court requirements.
- Standard outpatient often fits maintenance and step-down care. It gives people a place to keep working on depression, recovery skills, and medication follow-up after they have gained more footing.
That practical fit matters. A treatment plan only helps if the person can get there, attend regularly, and keep showing up even on a hard week.
How therapy and medication fit together
Therapy helps people do more than talk about problems. It teaches them how to interrupt the loop between painful thoughts, emotional shutdown, cravings, and impulsive choices. Cognitive behavioral therapy is one common approach. It helps a person notice the thought patterns that drive both depressed mood and substance use. Other skills-based approaches focus on emotional regulation, communication, stress tolerance, and relapse prevention.
Medication can also be part of the plan. For opioid use disorder, medication-assisted treatment may include options that reduce withdrawal symptoms and cravings. For depression, prescribing decisions should account for current substance use, recent abstinence, sleep, energy, safety concerns, and how severe the mood symptoms are. The same research noted earlier found that medication response in this population can differ from what clinicians often see in depression alone, which is one reason careful follow-up matters.
No medication fixes this by itself.
The goal is a treatment plan that is realistic, coordinated, and workable in everyday life. For someone in Dallas, Fort Worth, Euless, Arlington, or the surrounding area, that often means choosing a level of care that matches both clinical needs and practical realities like transportation, work hours, family responsibilities, and insurance. The best starting point is usually the option a person can attend consistently and build on over time.
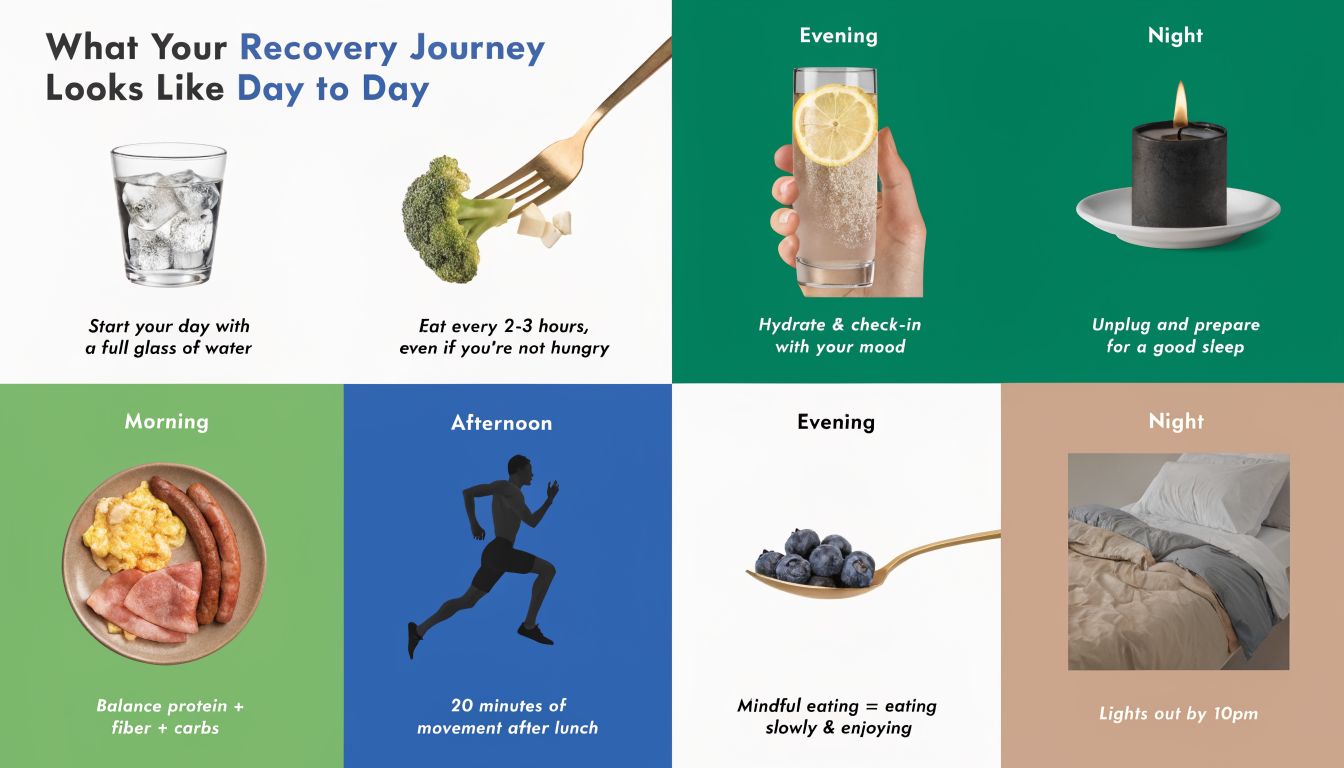
What Your Recovery Journey Looks Like Day to Day
Fear of treatment often comes from not knowing what a normal day will feel like. Families worry about whether the setting will be cold, intense, or impersonal. Many people entering outpatient care expect judgment. What helps most is knowing that structured treatment usually feels much more human and steady than people imagine.
The first few days
The process usually starts with an intake assessment. Staff gather information about substance use, mood symptoms, safety concerns, medical history, family stressors, and practical needs like schedule and transportation. That first step isn’t about catching someone saying the wrong thing. It’s about building a plan that fits the person’s actual life.
Soon after intake, the person typically receives a treatment schedule and begins meeting with clinicians. Some sessions are individual. Others are group-based. If medication support is appropriate, medical providers discuss options and monitor how the person responds.
What a treatment day often includes
A typical outpatient day depends on the level of care, but it often includes a mix of focused therapeutic work and practical recovery support.
- Check-in and goal setting. The person may review mood, cravings, sleep, stressors, and any recent substance use.
- Group therapy. Clients often talk through triggers, coping skills, family conflict, shame, relapse warning signs, and how to manage emotions without using.
- Individual therapy. One-on-one sessions create room for private topics such as grief, trauma, relationship strain, or persistent depressive thoughts.
- Skills and routine building. Many programs include work on structure, nutrition, sleep habits, stress management, and healthy communication.
People are often surprised by group therapy. They expect pressure or embarrassment. Instead, many find relief in hearing others describe the same thought loops, the same hiding, and the same fear about starting over.
Recovery often becomes more believable when a person hears someone else say out loud what they’ve been trying to hide.
The environment matters too. A calm outpatient setting can help people practice recovery while still engaging with their everyday lives. They leave session, return home, and start using new skills in actual situations with family, work stress, cravings, and ordinary routines. That’s one reason outpatient care can be such a practical fit for people in Dallas and Euless who need support that carries directly into daily life.
Making Treatment Accessible Navigating Insurance and Costs
A lot of families in Dallas-Fort Worth reach this point at night, after everyone else is asleep, staring at an insurance card and wondering what treatment will cost. The fear is rarely just the bill itself. It is the fear of starting something they cannot afford to finish, or calling for help and still not getting a clear answer.
That uncertainty can keep people stuck longer than they need to be.
For depression and substance use treatment, the first financial step is usually simple. Ask for an insurance verification and a plain-language review of benefits. Families often expect a maze. A good admissions team should give them a map. They should be able to explain what the plan may cover, what level of outpatient care fits the situation, and whether there may be out-of-pocket costs.
Why cost questions feel so heavy
Money stress and treatment stress tend to pile on each other. A parent may be worried about copays, a young adult may be worried about missing work, and a spouse may be wondering how to manage school pickup, commutes across DFW, and weekly appointments. Those are real barriers, not excuses.
Depression adds another layer. It can make basic tasks feel harder, including phone calls, paperwork, and decisions. Substance use often adds urgency, but not always clarity. Families can end up frozen, even when everyone agrees help is needed.
What to ask on the first call
It helps to treat the first conversation like gathering directions before a long drive across the Metroplex. You do not need every answer at once. You just need the next few turns.
Ask:
- What outpatient levels of care does my insurance appear to cover? This helps clarify whether standard outpatient, IOP, or PHP is the likely fit from a benefits standpoint.
- What costs should we plan for right away? Ask about deductibles, copays, coinsurance, and any fees that may not be covered.
- How often would treatment meet each week? This matters for work schedules, childcare, and transportation.
- Can someone explain this in plain language? If the answer sounds like insurance jargon, ask again. Clear programs expect that question.
- What if we do not have good coverage? Some programs can discuss self-pay options or other practical next steps.
Families often feel relief after this call because the problem becomes concrete. Concrete problems are easier to solve.
If you want a clearer picture before you reach out, this guide on insurance coverage for mental health treatment and addiction rehab explains common questions in straightforward terms.
Practical realities for DFW families
In North Texas, access is not only about price. It is also about time and distance. A program may be clinically appropriate but still hard to attend if the drive conflicts with rush hour on I-30, I-35, or 183, or if a family is trying to coordinate work, school, and home responsibilities. That is one reason outpatient care can make sense. It lets people get structured help while staying connected to daily life.
Ask about scheduling early. Evening hours, location, and frequency of sessions can matter just as much as the insurance quote. A treatment plan only helps if a person can show up for it.
The goal is not to solve every financial and logistical detail in one day. The goal is to turn a vague fear into a short, workable checklist. That is often the moment treatment starts to feel possible.
Life After Treatment Building Lasting Recovery in DFW
A lot of families expect the hardest part to be getting someone into treatment. Then the program ends, everyone goes home, and a new question shows up fast. What helps recovery hold when real life starts again on Monday morning?
That phase matters because depression and substance use both tend to return under ordinary pressure. A rough week at work, conflict at home, long drives across DFW, isolation on the weekend, or missed sleep can all start to wear down the progress someone fought hard to build. Recovery after treatment works more like physical therapy after an injury than a one-time fix. The structured care did important work. Now the goal is to keep strengthening the habits and supports that protect that progress.
What strong aftercare usually includes
Good aftercare is usually a weekly routine, not a single follow-up call. It often includes a few pieces working together:
- Continued therapy. Regular counseling gives someone a place to catch mood changes, stress, and substance cravings early, while they are still manageable.
- Peer support. Alumni groups, recovery meetings, or other local support communities reduce isolation. They also remind a person that a setback is a signal to ask for help, not a reason to disappear.
- A written relapse response plan. This can include warning signs, coping steps, phone numbers, transportation options, and who should be contacted if symptoms or substance use return.
- Family clarity. Loved ones do better when they know what improvement looks like. Learning the stages of recovery after treatment can help families respond with steadiness instead of panic.
That last point is easy to miss.
Families often assume recovery should look smooth once treatment ends. In real life, it usually looks uneven. A person may do well for weeks, then have a hard stretch. That does not automatically mean treatment failed. It may mean the support plan needs to be used the way it was designed to be used.
Why local connection matters in North Texas
In DFW, aftercare has to fit real schedules or it often falls apart. A plan may sound solid on paper, but it will not help much if the drive from Euless to Dallas turns a therapy visit into a two-hour commitment, or if group times collide with work, school pickup, or probation requirements.
Local support changes that. When care is close enough to attend consistently, people are more likely to keep therapy appointments, return quickly after a missed week, involve family, and ask for help before a lapse becomes a full relapse. Convenience is not a small detail here. It is part of what makes long-term recovery realistic.
Recovery in North Texas often depends on simple, practical questions. Can this person get there after work. Is the schedule manageable. Does the family know who to call if depression worsens on a Sunday. Is there enough structure to keep the week from drifting.
Families in Euless, Dallas, and the wider metroplex do not have to figure all of that out alone. Maverick Behavioral Health provides outpatient care for substance use, depression, and other co-occurring conditions through PHP, IOP, standard outpatient services, and MAT support. To ask questions, verify insurance, or talk through next steps, call (888) 385-2051.