


When addiction has turned daily life into crisis management, individuals often don’t need a lecture. They need a map. A spouse may be watching promises get broken again. A parent may be scanning every text message for signs something is wrong. A person struggling with alcohol or drugs may wake up wanting change, then feel overwhelmed before breakfast.
That confusion is common. Recovery can feel huge when it’s viewed as one giant leap. It becomes more manageable when it’s understood as a series of stages.
The stages of recovery give language to what many families already sense. There’s a point where someone begins to see the problem. There’s a point where the body and brain need stabilization. There’s a point where deeper emotional work begins. Then there’s the long stretch of protecting progress and building a life that feels worth staying sober for.
Recovery also isn’t a straight line. In the Transtheoretical Stages of Change Model, people often need a mean of 5.35 serious recovery attempts before resolution, which helps explain why returning for help can be part of the process, not proof that change is impossible (research on serious recovery attempts).
That matters for families in Euless and across Dallas-Fort Worth. It means a setback doesn’t erase hope. It means treatment should match the stage a person is in, not the stage everyone wishes they were in. It also means practical support, structure, and patience can make a real difference.
Table of Contents
- The Roadmap A Framework for the Stages of Recovery
- Laying the Foundation Early Recovery and Stabilization
- Building the Walls Middle Recovery and Rehabilitation
- Living in the House Long-Term Maintenance and Aftercare
- Navigating Storms Relapse Warning Signs and Prevention
- Begin Your Journey Today at Maverick Behavioral Health
The Roadmap A Framework for the Stages of Recovery
A family often arrives with the same urgent question. “What happens first, and how do we know what kind of help is needed now?” That question matters because recovery is not one decision followed by automatic progress. It unfolds in phases, and each phase calls for a different kind of support.
A simple way to picture the process
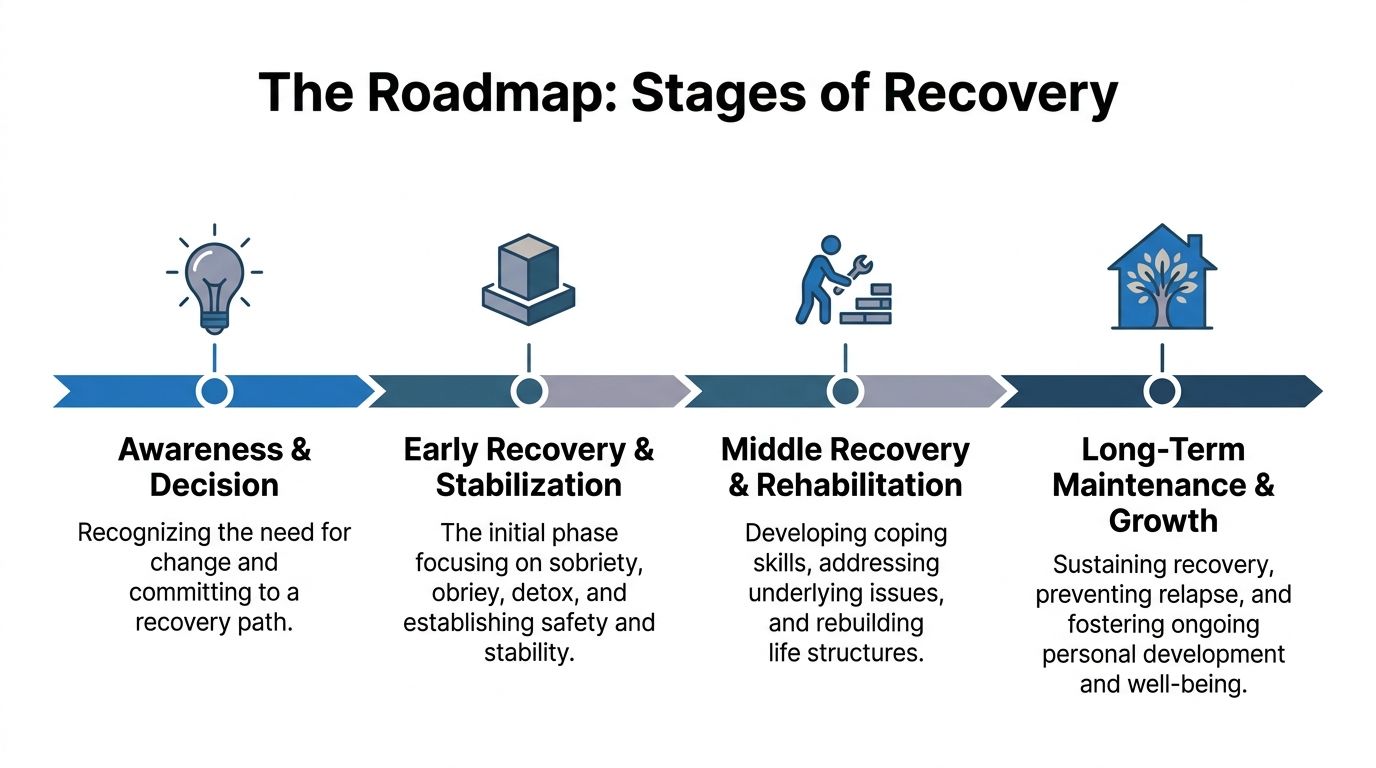
Four broad phases give patients and families a practical map.
| Stage | Main task | What it often feels like | Support that may fit |
|---|---|---|---|
| Awareness and decision | Admitting change is needed | Ambivalence, fear, relief, resistance | Assessment, honest conversation, treatment planning |
| Early recovery and stabilization | Getting safe and sober | Fatigue, cravings, mood swings, uncertainty | Higher structure, medical support, PHP, MAT when appropriate |
| Middle recovery and rehabilitation | Learning how to live differently | Effort, grief, growth, rebuilding | Therapy, group work, skill building, IOP |
| Long-term maintenance and growth | Protecting progress | More confidence, but ongoing vigilance | Aftercare planning, continued counseling, recovery routines |
This model is simple, but it helps people stop treating recovery like a pass or fail test. The process is closer to physical rehabilitation after an injury. First you reduce immediate danger. Then you rebuild strength, coordination, and trust in your body. Lasting change comes from repeating the right supports long enough for them to become part of daily life.
People often feel discouraged when progress is uneven. That discouragement usually comes from expecting a straight path. Recovery rarely works that way. Motivation can rise and fall, symptoms can change from week to week, and a return to treatment may reflect renewed honesty rather than failure.
Recovery often moves in loops. Returning for help can mean the person is still choosing change.
How the stages connect
Each stage has its own job. In the beginning, the goal is recognition. A person starts to see that substance use is causing harm, even if another part of them still wants to keep using. That inner conflict is common. It does not mean treatment cannot work.
Once someone says yes to help, the focus shifts to stabilization. The brain and body need time, structure, and often medical guidance to settle down. At Maverick, a higher level of care such as PHP can provide daily support, while MAT can reduce cravings and withdrawal symptoms for people recovering from opioid or alcohol use disorders when clinically appropriate.
After stability improves, treatment can widen its focus. The work becomes less about getting through the next 24 hours and more about understanding patterns. Patients begin practicing coping skills, repairing relationships, and addressing depression, anxiety, trauma, or stress that may have kept substance use going. An IOP often fits this stage well because it gives steady therapeutic support while allowing a gradual return to work, school, or family responsibilities.
Long-term recovery asks a different question. How does a person keep healing while living real life? That phase includes maintenance, aftercare, community support, and a plan for setbacks before they happen. The level of care is lower, but the attention is still active.
The key idea is simple. Recovery support should match the stage a person is in. Someone in acute distress usually needs more structure than someone who is stable and practicing new routines. Maverick’s PHP, IOP, and MAT options in Euless and Dallas are designed around that principle, so care can adjust as a person reaches each new milestone.
Laying the Foundation Early Recovery and Stabilization
A family may expect relief as soon as substance use stops. Then the first sober week arrives, and their loved one is sweating, restless, irritable, exhausted, and asking why they still feel so bad. That experience can be frightening, but it is common in early recovery. The body has stopped taking in the substance. The nervous system has not fully reset yet.

Why the first months feel so intense
Early recovery often centers on stabilization. In plain terms, that means helping the brain and body settle enough for a person to think clearly, sleep more regularly, and stay engaged in treatment. The Substance Abuse and Mental Health Services Administration explains that withdrawal and early recovery symptoms can affect mood, concentration, sleep, and daily functioning, which is one reason close support matters during this stage (SAMHSA guidance on withdrawal and early treatment support).
A house analogy can help here. Detox is like getting through the fire. Stabilization is checking the wiring, repairing the smoke damage, and making the home safe to live in again. The immediate danger may be lower, but the structure still needs careful attention.
That is why a person may feel physically safer than they did a few days ago and still struggle with cravings, anxiety, flat mood, poor focus, or sudden anger. Those symptoms do not mean treatment is failing. They often mean the healing process is underway and still needs time.
Common early-recovery challenges include:
- Sleep disruption, which can make everything feel harder.
- Cue-based cravings tied to places, conflict, loneliness, or routines associated with use.
- Rapid mood shifts as the brain adjusts without the substance it had come to expect.
- Low concentration and mental fog, especially in the first weeks.
What structured support looks like
In this stage, treatment works best when support matches the level of instability.
A Partial Hospitalization Program (PHP) often fits people who need frequent clinical contact, a dependable daily schedule, and strong accountability without round-the-clock inpatient care. For many patients at Maverick Behavioral Health in Euless and Dallas, PHP creates a steady rhythm during the day while they practice getting through evenings and mornings with a treatment plan still in place.
Medication-Assisted Treatment (MAT) is also a key component for some patients, especially those recovering from opioid or alcohol use disorders. Medications such as buprenorphine, methadone, and naltrexone are supported by the National Institute on Drug Abuse because they can reduce withdrawal, lower cravings, and improve treatment retention when used as part of a full treatment plan (National Institute on Drug Abuse overview of medications for opioid use disorder). For a patient in early recovery, that can mean the difference between being overwhelmed by symptoms and being able to participate in therapy.
An Intensive Outpatient Program (IOP) may become the better fit once symptoms are more manageable and the person can tolerate fewer treatment hours each week. At that point, the goal is not only symptom relief. It is practicing recovery skills in real life while still returning to structured care several times a week.
That step-down approach matters. Maverick’s PHP, IOP, and MAT services are not separate tracks that ignore each other. They work more like stages of scaffolding around a building. As stability improves, the level of support can change without losing continuity.
Practical rule: Early recovery does not require a person to feel strong. It requires enough support to stay safe, keep showing up, and let the nervous system settle.
How families can help without taking over
Families often feel pulled in two directions. One path is constant monitoring. The other is emotional withdrawal out of exhaustion or fear. A steadier response usually works better.
Helpful support in early recovery often includes:
- Protecting routine by encouraging treatment attendance, meals, sleep, and follow-up care.
- Reducing avoidable conflict during the first unstable weeks.
- Keeping clear boundaries around money, substances in the home, transportation, and behavior.
- Learning what recovery looks like, so temporary symptoms are not mistaken for lack of effort.
Consistency matters more than perfection. Families who want a clearer picture of healthy support can review these benefits of family involvement in addiction recovery, especially when they are trying to help without slipping into control.
For many patients, early recovery is less about dramatic breakthroughs and more about repetition. Show up. Rest. Eat. Take medication as prescribed if MAT is part of care. Return the next day and do it again. That is how the foundation gets poured, one steady day at a time.
Building the Walls Middle Recovery and Rehabilitation
Once the body is more stable, treatment shifts. The question is no longer just, “How does this person stop using today?” The question becomes, “How does this person build a life that doesn’t keep collapsing under stress?”

From crisis control to skill building
Middle recovery is where people start rebuilding the structure of daily life. That includes work habits, time management, relationships, boundaries, honesty, and emotional regulation.
This stage can surprise families. They may think, “The substances are gone, so why is everything still so hard?” The answer is that addiction usually becomes woven into how a person copes, avoids pain, handles conflict, and seeks relief. When the substance is removed, those gaps become visible.
An Intensive Outpatient Program often fits this phase well because it lets people practice new skills in the world while still receiving substantial support. A client might attend therapy, group sessions, and skills work several days a week, then test those tools at home, at work, or in school.
That balance matters in Dallas-Fort Worth, where many adults need treatment that can work around jobs, parenting, or class schedules.
How therapy changes the pattern
Middle recovery is where therapy becomes practical. It isn’t just talking about feelings in the abstract. It’s learning what happens between a trigger and a decision.
Two approaches often help:
- Cognitive Behavioral Therapy focuses on the link between thoughts, emotions, and behavior. A person learns to spot thoughts like “I already ruined today” or “No one would understand anyway,” then challenge them before they turn into action.
- Dialectical Behavior Therapy teaches skills for distress tolerance, emotional regulation, and interpersonal effectiveness. That’s useful for people who feel everything intensely or shut down under stress.
A simple example shows how this works.
A person gets criticized at work. Before recovery, the chain might look like this: shame, anger, urge, use. In treatment, the chain gets interrupted. The person notices the shame, names it, regulates the body, calls a support person, and delays the impulse. That’s not glamorous, but it’s how relapse prevention often works in real life.
Therapy in this phase may also address co-occurring mental health concerns. Depression, anxiety, trauma symptoms, and unresolved grief can all keep pushing a person back toward substances if they aren’t treated directly.
Middle recovery asks for more than abstinence. It asks for replacement. Old coping tools have to be replaced with new ones that hold under pressure.
Why group support matters
People often underestimate group therapy until they sit in a room and hear someone else describe the exact thought they were too ashamed to say out loud.
Isolation is one of addiction’s strongest reinforcers. Group treatment pushes back against that. It helps people practice honesty, receive feedback, tolerate discomfort, and build sober connection.
Group work in this stage often helps with:
- Normalizing recovery struggles so shame has less room to grow.
- Practicing communication when conflict, apology, or boundary-setting is needed.
- Building accountability through regular contact with peers who notice changes.
- Creating a sober network that isn’t centered on using.
Middle recovery also includes practical rehabilitation. Some people need help rebuilding a weekly schedule. Others need to repair family trust, return to work slowly, or learn how to make it through weekends without chaos.
That’s why this phase is often less dramatic than early recovery but just as important. The walls of the new house are going up. If they’re thin, every future stressor blows through. If they’re solid, the person has a real chance to stay steady.
Living in the House Long-Term Maintenance and Aftercare
A few months after treatment, a person may look better to everyone around them. They are sleeping more regularly, showing up for work, and arguing less at home. Family members often feel relieved at this point. The confusing part is that recovery still needs steady care, even when the crisis has passed.

Maintenance requires continued practice
Long-term recovery works more like physical therapy after an injury than a finish line. Pain may be lower, and daily function may be better, but strength holds only if the person keeps using the muscles that support healing.
Researchers at the National Institute on Drug Abuse note that relapse rates for substance use disorders are similar to those of other chronic medical conditions, which is one reason aftercare matters so much over time (drug addiction treatment and relapse rates). That comparison can be reassuring. A return of symptoms does not mean treatment failed. It means the condition still needs management, support, and adjustment.
This stage is also where treatment becomes more individualized.
Some people need weekly therapy and medication management for a long stretch. Others do well with less frequent check-ins but need a plan for predictable stress points such as holidays, grief anniversaries, or job changes. At Maverick, that step-down process is not one-size-fits-all. A person who completed PHP may continue into IOP for structure and accountability, while someone benefiting from MAT may stay closely connected to medication follow-up as part of long-term support in Euless or Dallas.
What aftercare usually includes
A useful aftercare plan is specific enough to follow on a hard day, not just a good day. It should answer simple practical questions before stress gets high.
Strong aftercare often includes:
- Scheduled therapy appointments to track mood, cravings, trauma symptoms, and life stress.
- Ongoing peer support through recovery meetings or alumni connection.
- Medication follow-up for people using MAT, so cravings and withdrawal risk stay monitored.
- A written relapse response plan that spells out who to call, where to go, and how support increases quickly.
- Family guidance so loved ones know the difference between helping and overreacting.
For people leaving a higher level of care, Maverick’s aftercare support for ongoing recovery explains how treatment can stay structured even after the most intensive phase ends.
A good plan also has backup options. If work hours change, if transportation falls through, or if motivation drops, the person already knows what the next safe step is.
Why the brain still needs repetition
Families sometimes ask, “If treatment helped, why does my loved one still need meetings, therapy, or medication?” The short answer is repetition.
Addiction trains the brain through repeated reward, relief, and habit. Recovery retrains it the same way. Cognitive behavioral therapy helps people catch automatic thoughts, slow down impulsive reactions, and practice different responses often enough that those responses become more available under stress. For some patients, MAT adds another layer of stability by reducing cravings and helping the brain and body settle enough to use therapy well.
That is why maintenance can feel quieter than earlier stages while still doing heavy work. The brain is learning consistency.
Making sobriety livable
Long-term maintenance is not only about avoiding substances. It is also about building a life the person can stay in.
That may include a regular sleep schedule, meals that happen at normal times, exercise, repaired family routines, and friendships that do not revolve around chaos. It may also include learning ordinary but difficult skills, such as sitting with boredom, tolerating disappointment, or asking for help before things unravel.
Common anchors in this stage include:
- Daily routines that reduce drift and impulsive choices.
- Healthy relationships that support honesty instead of secrecy.
- Stress regulation skills such as breathing work, movement, journaling, or therapy homework.
- Meaningful roles at home, school, work, or in the community.
This is often where people begin to feel a deeper kind of hope. Not the shaky hope of “maybe I can stop,” but the steadier hope of “I know how to keep going, and I know where to turn if life gets hard again.”
Navigating Storms Relapse Warning Signs and Prevention
Relapse is often treated like a sudden event. In practice, it usually builds. The return to use may happen quickly, but the drift toward it often starts earlier in thoughts, emotions, routines, and relationships.
That distinction reduces shame. It also gives families and patients more chances to intervene.
Relapse is common in early recovery, with 40% to 60% of people relapsing in the first year. The encouraging part is that risk drops to below 15% after five years of continuous sobriety, which shows that vigilance and maintenance matter over time (recovery trajectories and relapse risk over time).
The warning signs usually come in clusters
The red flags often show up in three overlapping categories.
Emotional signs may come first. The person gets more irritable, restless, defensive, or numb. They may stop talking openly about stress. Sleep can worsen. Small frustrations start to feel outsized.
Mental signs often follow. The person starts bargaining internally. They remember the relief of using but forget the consequences. They may glamorize old routines, minimize past damage, or think in all-or-nothing ways such as, “If this week is already bad, nothing matters.”
Behavioral signs are usually easier for family members to see. Meetings get skipped. Therapy feels optional. Calls go unanswered. The person starts spending time with unsafe people, revisiting old places, or isolating behind closed doors.
A short checklist can help:
- Watch for withdrawal from support, structure, and honest conversation.
- Notice secrecy around schedules, money, phones, or whereabouts.
- Take mood changes seriously when they come with isolation or defensiveness.
- Pay attention to routine collapse such as sleep reversal, missed work, or skipped treatment.
The earliest warning sign is often not craving. It’s disconnection.
What to do at the first sign of trouble
Families often wait too long because they don’t want to overreact. A faster response is usually safer.
Useful actions include:
- Name the concern clearly. Calm statements work better than long confrontations.
- Reduce access to high-risk situations. That might mean changing plans for the evening or avoiding a triggering environment.
- Reconnect with support the same day. Contact a therapist, treatment provider, sponsor, recovery group, or trusted family member.
- Increase structure immediately. More check-ins, more accountability, and less isolation can slow the slide.
- Return to treatment if needed. A higher level of care can be the right move when warning signs are stacking up.
Families looking for practical steps can use these relapse prevention strategies for staying sober after rehab in Dallas as a starting point for a concrete plan.
The most important reframe is this. Relapse risk doesn’t mean recovery isn’t working. It means addiction is a condition that requires attention over time. When warning signs are recognized early, people can often interrupt the process before a full return to use takes hold.
Begin Your Journey Today at Maverick Behavioral Health
By the time many people search for help, they’re already exhausted. The person using may be tired of trying to control it alone. The family may be tired of guessing what to say, what not to say, and whether the next phone call will bring relief or bad news.
A stage-based view of recovery helps because it replaces panic with direction.
If someone is still in denial or ambivalent, the immediate job is engagement and honest assessment. If the person is in the first fragile stretch of sobriety, stabilization matters most. If the crisis has eased, treatment can move into deeper therapy, coping skills, and rebuilding. If formal treatment is ending, aftercare and maintenance become the priority.
That’s why matching care to the person’s stage matters so much. PHP can help when a person needs significant day-to-day structure. IOP can support people who are ready to practice recovery while staying connected to work, school, or family life. MAT, including Suboxone for appropriate opioid cases, can reduce withdrawal and cravings so the person has a fair chance to stay engaged. Standard outpatient care and aftercare planning help protect gains over the long run.
For adults in Euless, Dallas, and the surrounding Dallas-Fort Worth area, that kind of step-by-step care can make recovery feel less abstract and more doable. The process doesn’t have to be perfect to be real. It has to be supported, honest, and sustained.
Families should also remember something simple but important. The person they love doesn’t need to have every answer before making the call. They don’t need a perfect speech, a perfect level of readiness, or a perfect plan. They need the next right step.
Recovery usually begins that way. One conversation. One assessment. One day of showing up. Then another.
Your roadmap to recovery is here. You don't have to walk it alone. Call (888) 385-2051 to speak confidentially with a care coordinator and take the first step.
Maverick Behavioral Health provides outpatient addiction and mental health treatment for adults in Euless and the Dallas-Fort Worth area, including PHP, IOP, standard outpatient care, dual diagnosis treatment, MAT, and aftercare planning. People who are ready to explore the next step can visit Maverick Behavioral Health or call (888) 385-2051 for a confidential conversation about admissions.