


A lot of Dallas-Fort Worth families reach this search in the same state. One hand is holding a Blue Cross Blue Shield card. The other is holding together a situation that already feels like too much. Someone needs help for pills, alcohol, fentanyl, meth, or another substance. Work is being missed. Sleep is gone. Nobody has time to decode insurance language while a crisis gets worse.
The good news is simple. Blue cross blue shield drug rehab coverage is real, widely used, and often much better than families assume. In fact, over 17,000 people have used Blue Cross Blue Shield insurance to attend treatment at American Addiction Centers’ facilities since 2020. That matters because it shows BCBS isn’t some unusual or difficult option in addiction care. It’s one of the most commonly used paths into treatment.
For people in Euless, Dallas, Fort Worth, Arlington, Grapevine, Bedford, Irving, and the surrounding metroplex, the issue usually isn’t whether coverage exists. The issue is figuring out what level of care fits the situation, what the plan will approve, and how to move fast without making expensive mistakes.
Table of Contents
- Navigating Your Path to Recovery with BCBS in Texas
- The Key Terms in Your BCBS Drug Rehab Policy
- Decoding BCBS Coverage for Different Levels of Care
- Prior Authorization and Medical Necessity Explained
- How to Verify Your Benefits and Get Treatment Authorized
- Appealing a Denial from Blue Cross Blue Shield
- Why DFW Residents Choose Maverick with Their BCBS Plan
- Common Questions About Using BCBS for Addiction Treatment
Navigating Your Path to Recovery with BCBS in Texas
A common DFW scenario looks like this. A spouse is searching from the car in a parking lot. A parent is waiting until everyone else is asleep. An adult child is trying to help from another city while asking a simple question that feels impossible to answer under pressure. “What will Blue Cross Blue Shield cover?”
That question deserves a clear answer, not a runaround.

In Texas, BCBS coverage can open the door to several types of addiction treatment, including outpatient care, therapy, and medication support when a clinician documents the need. That’s the part families often miss. Insurance approval usually turns on clinical need and plan rules, not on who sounds most desperate on the phone. Desperation is understandable. Documentation is what gets decisions made.
Practical rule: The fastest way to calm the chaos is to stop guessing about coverage and start verifying the exact plan benefits tied to the member ID card.
Families in Euless and across Dallas-Fort Worth also need a local lens. Rehab searches get confusing when every website sounds the same and none of them explain what this means for someone who has to keep working, get home for the kids, or manage a co-occurring mental health condition. Local outpatient care matters because many people don’t need to leave the metroplex to get structured treatment.
For many Texans, BCBS is not the obstacle. The primary obstacle is delay. Waiting for “proof” that things are bad enough usually makes the situation worse. Calling for a benefits check and clinical screening is usually the smartest next move because it turns a vague insurance question into a treatment plan with actual options.
The Key Terms in Your BCBS Drug Rehab Policy
Insurance language feels intimidating because it’s built around billing, not plain English. A better way to think about it is a car repair bill. The shop doesn’t just say “covered” or “not covered.” There’s the amount paid before coverage starts, the share paid at each visit, and the cap on how much the customer pays in a plan year.
That same logic drives blue cross blue shield drug rehab coverage.
Deductible
A deductible is the amount the member usually pays before the plan starts sharing more of the cost for covered services. If the deductible hasn’t been met, the member may owe more upfront for treatment-related services.
This is the number families should ask about early because it affects the first bill more than almost anything else.
Copay
A copay is a fixed amount tied to a visit or service. In practice, a plan might assign a set charge for a therapy session, medication visit, or other covered outpatient service.
Copays are easier to budget for than most insurance costs because they’re predictable.
Coinsurance
Coinsurance is the member’s share of the allowed cost after the deductible has been met. Instead of a flat amount, it’s a percentage share of covered services based on plan terms.
This is why two BCBS members can get the same level of care and still owe different amounts. The plan design matters.
Insurance isn’t just about whether treatment is covered. It’s about how the cost gets split.
Out-of-pocket maximum
The out-of-pocket maximum is the ceiling on what a member pays for covered services in a plan year under the plan’s rules. Once that limit is reached, the plan typically pays more fully for covered care for the rest of that period.
This is one of the most useful numbers on the policy because it helps families understand worst-case financial exposure for covered treatment.
Why these terms matter before any admissions call
A lot of families ask the wrong first question. They ask, “Do you take BCBS?” That’s not enough. A better question is, “What does this specific BCBS plan cover for this specific level of care, and what would the member likely owe?”
Those are different questions, and the second one is the one that protects a family from surprises.
A simple checklist helps:
- Check the plan type: HMO, PPO, marketplace, employer-sponsored, and other plan structures can affect network rules and referral requirements.
- Confirm the deductible status: A plan may cover treatment, but current deductible status still affects immediate cost.
- Ask about outpatient behavioral health benefits: Many families are specifically looking for structured day or evening care, not just inpatient rehab.
- Verify authorization requirements: Some services need approval before treatment starts.
- Request an estimate in plain language: Families need a usable answer, not an insurance script.
A family doesn’t need to master insurance to get help. It just needs the right questions asked in the right order.
Decoding BCBS Coverage for Different Levels of Care
Not every person struggling with addiction needs the same setting. Some need medical stabilization first. Some need a full residential environment. Others need strong outpatient structure while continuing to live at home in Dallas-Fort Worth. BCBS decisions usually depend on medical necessity, the intensity of symptoms, and whether the requested level of care matches the actual clinical picture.
This continuum is easier to understand visually.
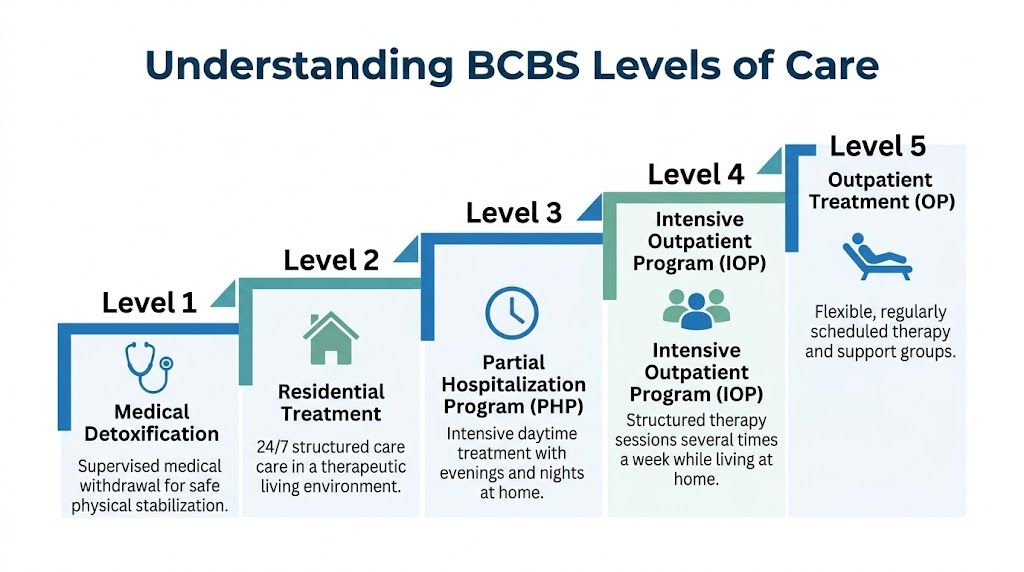
Medical detox
Medical detox is the front end of treatment when someone needs supervised withdrawal and physical stabilization. This level is usually appropriate when withdrawal risks are significant, when symptoms need monitoring, or when a person can’t safely stop using without medical support.
BCBS typically looks for clear evidence that detox is medically necessary, not just preferred. That may include the substance involved, withdrawal history, current symptoms, and safety concerns documented by a licensed provider.
A practical way to think about detox is this. It addresses immediate physical risk. It does not solve the addiction by itself. Families often want detox to be “the program,” but it’s really the first step when withdrawal is the urgent problem.
Residential treatment
Residential treatment provides a live-in environment with around-the-clock structure. This level may fit people who need separation from a high-risk environment, close monitoring, or intensive therapeutic support after detox or during a severe relapse pattern.
BCBS often requires strong clinical justification for residential care because it’s more intensive than outpatient treatment. If someone can remain safe at home and participate in structured outpatient services, the plan may approve a lower level instead.
That’s frustrating for families, but it’s also predictable. The insurer asks whether 24-hour supervision is necessary. If the answer is no, the plan may direct the member toward PHP or IOP instead.
Partial hospitalization program
PHP is one of the most important treatment options for DFW residents who need serious support without overnight stay. It offers intensive daytime treatment while the client returns home in the evenings.
For outpatient programs like PHP at 20+ hours per week and IOP at 9+ hours per week, BCBS coverage is generally tied to medical necessity, and those structured programs have been shown to reduce hospital readmission by 35% according to this BCBS coverage overview for substance abuse treatment levels.
PHP often makes sense when standard weekly therapy isn’t enough, but full inpatient treatment isn’t clinically required. It can be a strong fit for people stepping down from detox or residential care, and for people who need daily accountability, psychiatric support, relapse prevention work, and routine.
Intensive outpatient program
IOP is structured treatment several times each week while the client continues living at home. This level is often the most realistic answer for working adults, students, and parents in Euless, Dallas, Fort Worth, and nearby communities who need more than basic outpatient counseling.
BCBS usually wants to see why IOP is the right intensity. The documentation often needs to show ongoing substance use risk, relapse history, functional impairment, or failed attempts at lower levels of care.
A useful comparison:
| Level of care | Best fit |
|---|---|
| Weekly outpatient | Mild symptoms, strong stability, lower relapse risk |
| IOP | Moderate symptoms, repeated setbacks, need for frequent therapy and accountability |
| PHP | Higher acuity, unstable early recovery, need for near-daily structured treatment |
IOP is often where recovery becomes workable for people with real-world responsibilities. It gives structure without removing someone entirely from daily life.
The right level of care isn’t the most dramatic one. It’s the one a clinician can justify and the patient can actually complete.
Medication-assisted treatment with Suboxone or methadone
For opioid use disorder, medication-assisted treatment can be the difference between unstable recovery and a real chance at safety. BCBS plans are required to cover MAT such as buprenorphine and methadone when clinically appropriate, and clinical benchmarks cited by American Addiction Centers note that MAT decreases overdose mortality by 50% during the first year post-treatment and lowers relapse rates by 40% to 60% compared with detox alone in their Blue Cross Blue Shield MAT coverage discussion.
That’s why families should stop treating MAT like a backup plan. For many opioid cases, it should be part of the first serious conversation.
BCBS typically expects several things before approving MAT-related care:
- A licensed diagnosis: The chart has to document substance use disorder clearly.
- A treatment plan: The provider needs to outline medication strategy, counseling frequency, and clinical goals.
- Proof of medical necessity: The request has to connect treatment to the patient’s symptoms, risks, and history.
- Ongoing monitoring: Insurers want to see that care is active, not casual or open-ended.
MAT works best when it’s paired with counseling, accountability, and treatment for co-occurring mental health symptoms. It’s not trading one problem for another. It’s medical treatment for a high-risk disorder.
Prior Authorization and Medical Necessity Explained
Insurance approval can feel arbitrary when families are under pressure. It usually isn’t arbitrary. It’s bureaucratic, often slow, sometimes maddening, but still built around specific rules. Two of the biggest are medical necessity and prior authorization.

What medical necessity really means
Medical necessity means the requested treatment must match the person’s clinical condition. The plan wants evidence. It wants a diagnosis, symptom severity, risk factors, history, and a clear explanation of why this level of care is appropriate right now.
That’s why the same insurance company can approve one person for PHP and another for IOP. The decision is supposed to follow the clinical record.
A strong medical necessity review usually considers:
- Current substance use pattern: What’s being used, how often, and what risk it creates
- Withdrawal or relapse history: Recent instability matters
- Mental health concerns: Anxiety, depression, trauma symptoms, and other co-occurring issues can affect approval
- Daily functioning: Work, school, family stability, and safety all count
- Response to prior treatment: Failed lower levels of care can support a higher one
Why prior authorization matters so much
Prior authorization is the insurer’s approval process before certain services begin. Families often hate it because it sounds like a delay tactic. Sometimes it is slow. But in practical terms, it’s the checkpoint where the clinical team submits documentation and the plan decides whether it agrees with the requested care.
When prior authorization is required, skipping it can create major billing problems. That’s one reason families should read a plain-language explanation of pre-authorization before entering rehab.
A denial based on missing authorization is an administrative problem. A denial based on weak clinical documentation is a different problem. Both can be addressed, but they need different fixes.
How parity law protects access
Federal law gives families more protection than many realize. The Mental Health Parity and Addiction Equity Act requires insurers like BCBS to provide equal coverage for substance use disorder treatment as they do for medical services. It also means marketplace and group plans can’t impose more restrictive financial requirements or treatment limits on mental health benefits, as explained in this overview of parity and BCBS addiction coverage.
That doesn’t mean every request gets approved. It means the insurer has to use comparable standards when evaluating addiction treatment. If a plan would cover medically necessary care for a physical condition, it can’t create harsher coverage rules just because the condition is substance use disorder.
That protection matters. Families shouldn’t approach BCBS as if addiction care is some optional extra. It’s healthcare.
How to Verify Your Benefits and Get Treatment Authorized
Families usually waste time in one of two ways. They either avoid the call because they’re overwhelmed, or they call the insurance company without the information needed to get a usable answer. A better approach is direct and organized.
Start with the insurance card
The insurance card is the starting point because it gives the member ID, customer service contact, and often the plan name. Families should also have basic clinical facts ready, including the substance involved, any recent treatment, and whether the person is looking for outpatient care, MAT, or a higher level of support.
If the person has multiple policies or recently changed jobs, that needs to be clarified early. Eligibility mistakes create avoidable delays.
Choose the fastest verification route
Calling BCBS directly is one option. Calling a treatment admissions team is usually easier because the family gets both insurance guidance and treatment screening in the same process.
The practical advantage of provider-led verification is simple. The admissions team knows what benefit questions matter for treatment and can move from benefits review into the next authorization steps. Families who want a clearer idea of the process can review how to find out if insurance will pay for treatment.
A clean verification process usually asks for:
- Member information: Name, date of birth, member ID, and policy holder details
- Plan basics: Whether the coverage is active and what behavioral health benefits apply
- Network status: Whether the provider is in network or how out-of-network benefits work
- Authorization rules: Whether pre-approval is needed for the proposed level of care
- Expected costs: Deductible status, likely member responsibility, and any visit-based cost sharing
What happens after benefits verification
Benefits verification is not the same thing as treatment approval. It confirms what the policy may cover. The next phase is clinical review.
That usually includes a screening or assessment, provider recommendations, and submission of documentation if prior authorization is required. The insurer then reviews the case against its criteria for the requested level of care.
A simple way to keep the process moving is this:
- Gather the card and demographics
- Confirm active coverage
- Complete a clinical assessment
- Match the patient to the right level of care
- Submit authorization if required
- Review expected out-of-pocket costs before admission
Families don’t need to solve each step alone. They do need to act quickly. Waiting for the situation to become “serious enough” is one of the most expensive decisions people make in addiction care.
Appealing a Denial from Blue Cross Blue Shield
A denial feels personal when a family is scared. It usually isn’t. It’s a claims decision, and claims decisions can be challenged. The most important thing is not to treat the denial letter like the end of the road.
The denial is not the final word
There are generally two levels of review when a request is denied. The first is an internal appeal, where the insurer reviews the decision again. If that doesn’t resolve the issue, an external review may be available depending on the plan and the type of denial.
The denial notice usually states why the request was rejected. That reason matters. Some denials are about missing paperwork. Others are about the insurer concluding that a lower level of care is sufficient.
What usually strengthens an appeal
A strong appeal is specific. It doesn’t argue that the family is upset, even though that’s understandable. It argues that the clinical facts support the requested care and that the original decision missed or misread those facts.
The most useful appeal materials often include:
- A more detailed clinical summary: Symptom severity, relapse pattern, safety concerns, and functional impairment
- Treatment history: Prior attempts, recent setbacks, and why lower-intensity care isn’t enough
- Provider recommendation: A direct statement of why the requested level is medically necessary
- Administrative cleanup: Correct forms, dates, and records submitted on time
Families facing that situation should review how to seek a second opinion or appeal a rehab insurance denial.
A denial means the case needs a stronger argument or cleaner paperwork. It does not mean the person doesn’t need help.
Why DFW Residents Choose Maverick with Their BCBS Plan
A Fort Worth parent gets off work, looks at a Blue Cross Blue Shield of Texas card, and needs an answer tonight. They cannot disappear for 30 days. They still need to keep a job, pick up the kids, and start treatment before the next relapse turns into an ER visit or another lost week. That is why many DFW families choose local outpatient care in Euless instead of chasing a program hours away.
Maverick Behavioral Health serves Dallas-Fort Worth with outpatient addiction and mental health treatment built for real life. For people using a BCBS plan, the fit often comes down to the levels of care families ask about most: PHP, IOP, standard outpatient care, dual diagnosis treatment, and MAT with Suboxone. If someone needs structure during the day but does not need an overnight stay, those services make sense.
Location matters more than families expect. Euless is practical for people coming from Dallas, Fort Worth, Arlington, Bedford, Irving, Grapevine, and nearby cities. A shorter drive makes it easier to keep showing up, and showing up is what keeps treatment working.
Families also choose Maverick because admissions support matters. You should not have to decode your BCBSTX benefits alone while your loved one is in crisis. A good admissions team helps confirm outpatient benefits, explain likely out-of-pocket costs, and sort out the next step without adding confusion.
If you live in DFW and want to use your BCBS plan for outpatient addiction treatment, call (888) 385-2051 for a free, confidential benefits check. You can also learn more about services at Maverick Behavioral Health.
Common Questions About Using BCBS for Addiction Treatment
Can an out-of-state BCBS plan be used in Texas
Often, yes. But it depends on the specific plan’s network and benefits. Families should never assume that a BCBS card from another state works the same way in Texas without verification. The smart move is to confirm network status, behavioral health benefits, and authorization requirements before scheduling treatment.
Is PPO or HMO better for rehab access
In practical terms, PPO plans are often easier to work with because they may offer more flexibility with provider choice. HMO plans may require tighter network use and more gatekeeping, such as referrals or stricter approval pathways. The exact plan rules matter more than the label alone, so verification is still essential.
Is a doctor referral always required
No. Some plans may require a referral, while others don’t. The answer depends on the policy and the level of care being requested. Families shouldn’t guess. They should ask directly during benefits verification because missing a referral requirement can delay care.
Will BCBS cover care for both addiction and mental health
Many plans do cover both, especially when the person has co-occurring symptoms that affect treatment needs. The key is proper diagnosis and documentation. When anxiety, depression, trauma symptoms, or other mental health concerns are part of the clinical picture, the treatment request should reflect that clearly.
What if someone wants outpatient care instead of inpatient rehab
That may be exactly the right fit. Many people in DFW need a structured outpatient program because they can remain safe at home, still need strong support, and can’t step away completely from family or work responsibilities. The right question isn’t whether outpatient sounds easier. It’s whether outpatient is clinically appropriate and covered under the plan.
Families in Dallas-Fort Worth don’t need to keep guessing about blue cross blue shield drug rehab coverage. Maverick Behavioral Health helps adults and families in Euless and the surrounding area verify BCBS benefits, understand likely costs, and move into the right outpatient level of care, including PHP, IOP, and MAT. For a free, confidential benefits check, call (888) 385-2051 today.