


Some people in Dallas-Fort Worth wake up already bargaining with themselves about alcohol. They promise that tonight will be different. They’ll stop at one drink. They’ll skip the liquor store. They’ll only drink on weekends.
Then stress hits. Or loneliness. Or boredom. Or a familiar thought shows up: “Just for tonight.”
By the end of the day, the same pattern repeats, followed by guilt, worry, and the fear that maybe nothing will work. Families feel it too. They see someone they love trying hard, then sliding back into the same routine.
That’s where cognitive behavioral therapy for alcohol addiction can be so helpful. It doesn’t ask people to rely on willpower alone. It teaches practical skills for understanding cravings, interrupting harmful patterns, and building a daily life that supports recovery. For working adults and students in places like Euless, Dallas, and the surrounding DFW area, that kind of structured, realistic help matters.
Table of Contents
- You Feel Trapped by Alcohol CBT Offers a Way Out
- Understanding the CBT Model for Alcohol Use
- Building Your Toolkit for Lasting Sobriety
- A Look Inside Your CBT Therapy Sessions
- Flexible CBT Programs for Your Life in Dallas-Fort Worth
- A Unified Approach to Recovery
- How to Start Cognitive Behavioral Therapy in Euless and Dallas
- Common Questions About CBT for Alcohol Addiction
You Feel Trapped by Alcohol CBT Offers a Way Out
It can look like an ordinary weekday in Dallas-Fort Worth. A college student drives back from class in Arlington already bargaining about drinking that night. A working adult in Euless finishes meetings, answers family texts, and still keeps one part of the mind focused on when alcohol will come next. From the outside, life may look organized. Inside, alcohol can start to set the schedule.
That trapped feeling is exhausting.
People often describe it as living with two systems running at once. One part of them wants relief, sleep, or a break from pressure. Another part feels scared, ashamed, or frustrated that drinking keeps taking up so much space. After enough promises to cut back, enough hidden bottles, or enough mornings spent regretting the night before, self-trust starts to wear down.

CBT offers a practical way out. It treats alcohol use as a pattern that can be observed and changed, much like tracing a traffic route that keeps leading to the same wrong exit. Once the route is clear, you can start building a different one.
That shift changes the whole conversation. Instead of blaming the person, CBT looks closely at what happens before the drink, during the urge, and after the alcohol wears off.
- What thoughts show up right before drinking
- What emotions make alcohol feel necessary
- What routines, places, or people strengthen the habit
- What skill could help in that exact moment instead
For a working adult in an evening IOP program, the pattern might begin with the drive home after a stressful commute on Highway 183, followed by the thought, “I need something to shut my brain off.” For a student balancing classes and work, it may start after an exam, a social event, or a lonely night in the apartment. In outpatient care, those real-life details matter because treatment has to fit the life the person is living, not a life put on pause.
A family may also feel trapped. Loved ones see promises made sincerely and broken sincerely. They may wonder whether therapy will be another conversation that sounds good for an hour but changes nothing by Friday night. CBT is designed to be more concrete than that. It gives people specific skills to practice between sessions, and in modern PHP and IOP settings, those skills are used while a person is still going to work, attending class, and managing home responsibilities.
CBT also fits well when alcohol use is tied to anxiety, depression, trauma symptoms, or sleep problems. It can be used alongside medication assisted treatment when that is appropriate. For many people in the Dallas-Fort Worth area, that combined approach is what makes treatment feel realistic. Care addresses the drinking, the mental health piece, and the demands of daily life at the same time.
CBT does not ask people to rely on willpower for every hard moment. It helps them practice a different response before the next hard moment arrives.
Hope usually starts there. Not with perfect confidence. With a workable plan, support that fits outpatient life, and a clear belief that patterns can change.
Understanding the CBT Model for Alcohol Use
A lot of people arrive at CBT with the same question. “I know drinking is hurting me, so why do I keep doing it?”
CBT answers that question with a model that is simple enough to follow in real life. Thoughts, feelings, and behaviors influence each other. In alcohol use, they can start working like a loop that repeats so often it feels automatic.
A common example looks like this. A person leaves work in Dallas after a draining commute on Highway 183, or a student heads home after class, work, and a pile of deadlines. The thought shows up fast: “I cannot do one more thing today unless I drink.” The body tightens. Stress rises. Drinking brings short relief. Then come the aftereffects, such as regret, conflict, poor sleep, or a harder morning. The next stressful moment arrives, and the brain remembers the same exit.
That repeated pattern is what CBT targets.
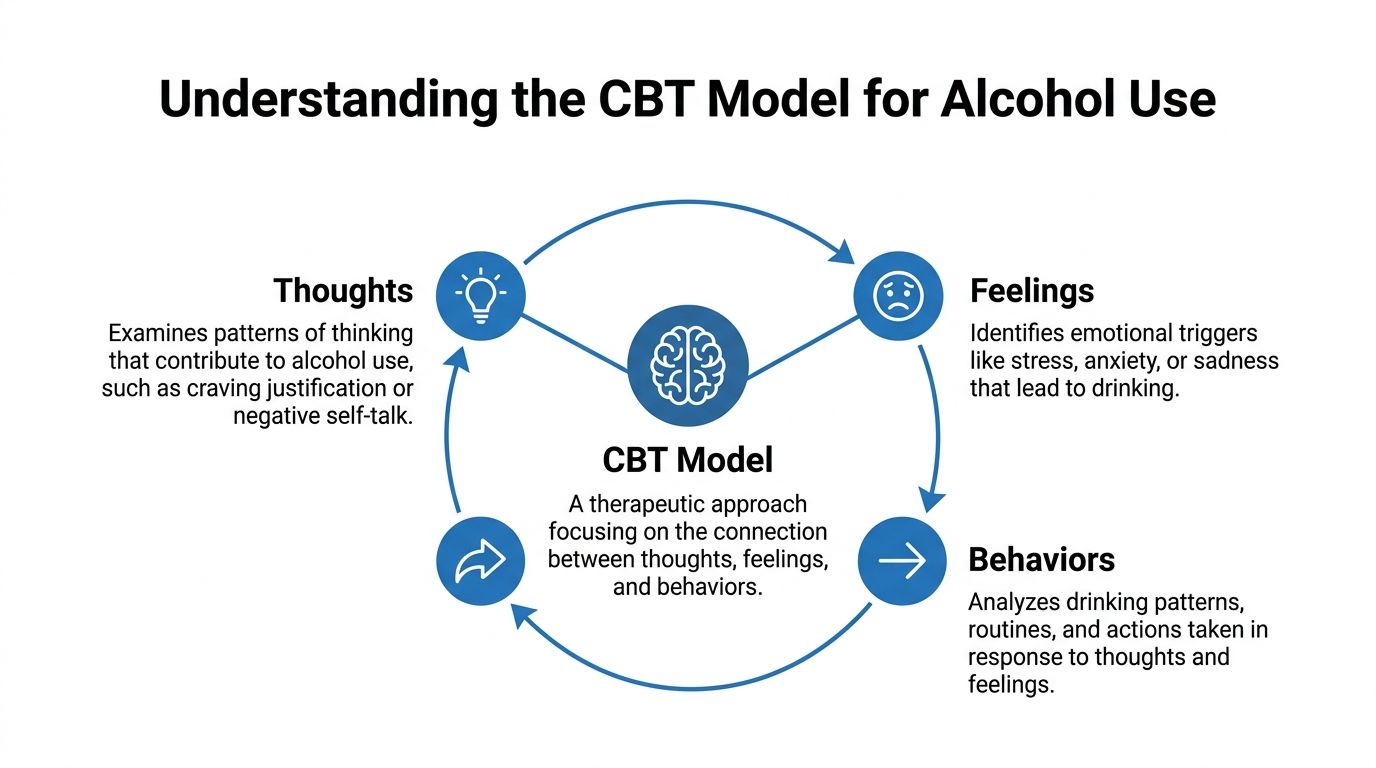
Thoughts can steer the whole cycle
Many alcohol-related thoughts happen so quickly that they feel like facts instead of mental habits. A person may not even notice them at first.
Common examples include:
- Permission thoughts such as “One drink will take the edge off.”
- Hopeless thoughts such as “I always end up here.”
- Relief thoughts such as “Alcohol is the only thing that slows my mind down.”
- All-or-nothing thoughts such as “I already slipped, so the day is ruined.”
CBT teaches people to slow that moment down and examine the thought instead of obeying it. A therapist might ask, “What else is true here?” or “What happened the last five times you told yourself that?” The goal is not forced positivity. The goal is accuracy.
That shift matters. Accurate thinking creates room for a different choice.
Feelings are real, but they do not have to run the plan
Alcohol use often grows around very human experiences. Stress. Shame. Anxiety. Anger. Loneliness. Emotional exhaustion. In dual-diagnosis treatment, those feelings are taken seriously because drinking may be tied to depression, trauma symptoms, panic, or sleep problems, not just habit alone.
CBT helps people sort out what they feel in the moment. That may sound small, but it changes treatment. Craving is handled differently than grief. Social anxiety is handled differently than irritability after a long day. When the problem gets a clear name, the response can become more precise.
In outpatient care, that precision matters because people are practicing these skills while still living real life. They are going to work, showing up to class, sitting in traffic, answering texts, and getting through family responsibilities the same week they are learning new responses.
Behaviors keep the pattern in place
Behavior is not only the act of drinking. It includes the setup.
A person may pass the same store every evening and stop without thinking. They may drink only after arguments, only when alone, or only when they cannot sleep. They may keep alcohol at home for “just in case” moments. Those routines can become as automatic as fastening a seatbelt.
CBT makes the sequence visible. Once the pattern is visible, it can be changed step by step. That might include changing a route home, planning the high-risk hour after work, removing alcohol from the apartment, or practicing coping skills for addiction triggers and stress before the urge peaks.
Why this model fits modern outpatient treatment
CBT works well in PHP and IOP settings because it is built for practice, not just insight. A working adult in Fort Worth may use it to prepare for client pressure, long drives, or drinking-centered work events. A college student in the Dallas area may use it to plan for weekends, exam stress, or the mix of isolation and social pressure that can fuel relapse.
It also fits well with a broader treatment plan. If someone is using medication for cravings or withdrawal support, CBT helps them handle the situations and thoughts that medication alone does not erase. If anxiety, depression, or trauma are part of the picture, CBT gives treatment a shared map so the drinking and mental health symptoms can be addressed together instead of in separate boxes.
Research has found that CBT for alcohol and other drug use disorders performs better than minimal or no treatment, as noted earlier in this article. That does not mean every person has the same experience. It means CBT has earned its place because it gives people a clear method for interrupting patterns that once felt fixed.
Families often find this model helpful too. Instead of seeing drinking as random or purely willful, they start to see the chain of stress, thought, feeling, and action around it. That understanding can lower blame and lead to more useful support at home.
Building Your Toolkit for Lasting Sobriety
CBT works best when it becomes practical. People don’t just talk about drinking. They learn skills they can use at home, in traffic, after work, at school, or during an argument.
That’s why many clinicians describe CBT as a toolkit. The goal isn’t to memorize therapy language. The goal is to have something useful ready when cravings, stress, or self-defeating thoughts hit.
People who actively use CBT coping strategies have shown a 40% reduction in alcohol-related relapse rates, and participants in CBT-based programs have demonstrated up to 30% higher treatment adherence than those in non-structured therapies, according to this Yale School of Medicine summary of digital CBT findings for alcohol use disorder.
How cognitive restructuring changes the story
Cognitive restructuring sounds technical, but the task is straightforward. It means learning to question thoughts that push drinking forward.
A common example looks like this:
- Trigger: A difficult email arrives from a supervisor.
- Automatic thought: “This day is ruined.”
- Feeling: Anxiety, anger, embarrassment.
- Urge: Drink after work.
- Behavior: Stop for alcohol on the way home.
In CBT, the person slows that chain down. They ask:
- Is this thought accurate
- What evidence supports it
- What evidence doesn’t
- What’s a more balanced thought
The original thought might become: “This email is stressful, but it doesn’t define the whole day. A reply can wait until there’s a clearer head.”
That shift doesn’t erase stress. It lowers the emotional intensity enough for a better choice to become possible.
How coping skills work in real life
Coping skills are the action side of CBT. They help people get through cravings and high-risk moments without reaching for alcohol.
One of the most useful exercises is a simple functional analysis. It looks at three pieces:
- What happened before the urge
- What happened during the drinking episode
- What happened after
A person might discover that the pattern is less random than it seemed. Maybe cravings rise after skipped meals, long commutes, and isolation. Maybe drinking temporarily reduces tension, but leads to arguments, poor sleep, and missed responsibilities.
That kind of map helps treatment get specific.
Some coping tools are immediate:
- Delay the urge: Set a short waiting period before acting on a craving.
- Change the environment: Leave the room, take a walk, or avoid a familiar drinking route.
- Reach out quickly: Text a trusted person before the craving becomes a plan.
- Use replacement behaviors: Eat, shower, journal, exercise, attend group, or practice a calming routine.
Some are longer-term. Building a stronger daily routine matters. Better sleep, predictable meals, supportive people, and planned sober activities reduce the chaos that often fuels drinking. For a deeper look at practical recovery skills, this guide on coping skills for addiction can help.
The best coping skill is the one a person uses in the moment.
How relapse prevention becomes a plan
Relapse prevention in CBT isn’t about fear. It’s about preparation.
People often assume relapse starts with the first drink. In practice, it usually starts earlier, with stress, isolation, secrecy, overconfidence, conflict, or a return to old routines. CBT helps clients identify those warning signs before alcohol enters the picture.
A relapse prevention plan usually includes:
- Personal triggers: certain people, places, emotions, and times of day
- Early warning signs: skipping meetings, minimizing stress, hiding cravings
- Protective actions: calling support, changing plans, increasing session attendance
- Emergency steps: what to do if drinking occurs or feels close
A good plan is concrete. “Do better” isn’t a plan. “Leave the event by 8 p.m., drive separately, and call support on the way home” is a plan.
Core CBT techniques for alcohol addiction
| Technique | Goal | Example in Action |
|---|---|---|
| Cognitive restructuring | Challenge distorted thoughts that justify drinking | A person replaces “I blew it, so I may as well keep drinking” with “One setback needs a response, not a surrender” |
| Functional analysis | Identify triggers, behaviors, and consequences | A client tracks what happened before and after a weekend binge to spot the pattern |
| Craving coping skills | Reduce the power of urges in the moment | Someone uses delay, distraction, and support contact during a strong evening craving |
| Refusal skills | Prepare for social pressure | A student practices a clear response before a party where alcohol will be present |
| Problem-solving | Address stressors that increase relapse risk | A working adult creates a plan for childcare and commute stress instead of drinking after overwhelm |
| Relapse prevention | Plan for high-risk situations and early warning signs | A client builds a weekend schedule to avoid isolation and unplanned drinking |
When CBT is working, people usually notice something important before they notice perfection. They gain a pause. There’s more space between urge and action. That space is where recovery grows.
A Look Inside Your CBT Therapy Sessions
Starting therapy can feel intimidating when someone doesn’t know what to expect. Many people worry they’ll be judged, pushed too hard, or asked to talk without direction.
CBT sessions are usually more structured than that. They tend to feel focused, collaborative, and practical.
What happens at the start of session
A typical session often begins with a brief check-in. The therapist may ask about drinking since the last meeting, current stressors, cravings, mood, and any urgent concerns.
The conversation usually has an agenda. That helps both people stay grounded. Instead of talking in circles, they choose what matters most that day.
For someone who’s nervous before treatment begins, this resource on how to prepare for your first therapy session can make the process feel more manageable.
What the middle of session feels like
The middle of session often focuses on one problem in detail. A therapist might help the client break down a recent drinking episode, identify the thoughts that came before it, and practice a different response.
In an individual session, that can look like careful problem-solving. In a group, it may involve hearing how others handled similar triggers and practicing a skill together.
A client might say, “I didn’t even think. I just drank.” The therapist helps slow that down. What happened an hour before? What feeling showed up first? What thought made drinking seem justified?
That kind of work can be emotional, but it’s also grounding. It gives shape to something that once felt chaotic.
Many people feel relief when they realize their drinking pattern can be understood instead of feared.
What happens before session ends
CBT usually ends with something concrete. The therapist and client decide what to practice before the next session.
That might include:
- Tracking triggers: writing down situations, thoughts, and urges during the week
- Practicing a response: using a coping statement or refusal skill in a planned setting
- Changing one routine: taking a different route home or removing alcohol from the house
- Reaching out intentionally: contacting support before a known high-risk time
This is often called homework, but it’s better understood as rehearsal. Recovery gets stronger when the skills leave the office and enter real life.
For families, this structure can be reassuring. The sessions aren’t random conversations. They’re guided opportunities to learn, practice, and make measurable progress one week at a time.
Flexible CBT Programs for Your Life in Dallas-Fort Worth
Many adults who need help with alcohol addiction also need to keep living their lives. They still have jobs, classes, children, deadlines, and responsibilities at home. That reality is one reason outpatient care matters so much in Dallas-Fort Worth.
CBT fits well in outpatient settings because it’s built around skill practice in daily life. People don’t just learn coping tools in session. They use them in the environments where drinking has become tied to routine.

Research also points to an important challenge. A review noted a gap in understanding how to best adapt CBT for part-time formats like IOP and PHP, and it highlighted how dropout can weaken results in these settings, as discussed in this review of CBT implementation challenges in outpatient substance use treatment. That’s why personalized scheduling and retention planning matter so much.
When PHP makes sense
A Partial Hospitalization Program, or PHP, offers a higher level of structure while still allowing a person to live at home. This level often fits people who need frequent clinical support but don’t need inpatient care.
PHP can help when someone has:
- Frequent cravings or relapse risk
- Significant emotional instability
- A recent step-down from a higher level of care
- A home life that’s stressful but still manageable with support
When IOP fits better
An Intensive Outpatient Program, or IOP, is often a strong match for working adults and students. It provides more support than weekly therapy while still leaving room for work, school, and family obligations.
IOP can be a practical option for people who need repeated contact, group support, and ongoing skill-building. Anyone trying to sort out whether this level of care fits can learn more about what IOP therapy is.
When standard outpatient care is enough
Standard outpatient therapy is usually less intensive. It may work well for someone with a stable living environment, solid motivation, manageable symptoms, and a lower immediate relapse risk.
This level can also be useful after PHP or IOP. A person may continue CBT in a less frequent format as they strengthen routines, relationships, and relapse prevention habits.
The key isn’t picking the most impressive level of care. It’s choosing the level that matches actual needs. For many people in Euless, Dallas, and surrounding communities, flexible outpatient treatment makes recovery possible because it fits real life instead of requiring life to stop.
A Unified Approach to Recovery
Alcohol addiction often overlaps with other problems. Depression can deepen isolation. Anxiety can intensify the urge to self-medicate. Sleep problems, trauma symptoms, and other substance use can all complicate the picture.
That’s why CBT works best when it’s part of a broader treatment plan rather than treated as a stand-alone fix.
CBT and dual diagnosis care
When someone lives with both alcohol use disorder and a mental health condition, treatment has to address both. If only the drinking is treated, the emotional pain underneath may keep pushing the cycle forward.
Reviews of studies on co-occurring alcohol use and depression found that integrated CBT was superior to usual care, according to this overview of CBT for substance misuse disorders and co-occurring concerns.
That matters in practical ways. A person with depression may need help identifying hopeless thoughts that increase drinking risk. A person with anxiety may need tools for panic, avoidance, and catastrophic thinking. If treatment targets only alcohol, the person may still feel trapped by the same internal pressure.
CBT and medication assisted treatment
Medication-assisted treatment can also play an important role in recovery, especially when cravings, withdrawal symptoms, or co-occurring opioid use are part of the clinical picture. Medication can support physical stability. CBT helps the person use that stability well.
These approaches do different jobs:
- Medication helps reduce physiological distress
- CBT helps change habits, beliefs, routines, and coping patterns
- Ongoing therapy helps people respond to setbacks without giving up
A person who feels less overwhelmed physically is often better able to absorb CBT skills. In turn, stronger CBT skills can help the person stay engaged with treatment, avoid high-risk situations, and handle stress without returning to alcohol.
Recovery is often strongest when biological support and behavioral support work together.
Families often find this integrated approach easier to understand than a one-track model. It acknowledges that alcohol addiction affects the body, the mind, relationships, and daily functioning all at once.
A modern outpatient plan may include individual therapy, group CBT, medication support when appropriate, and care for co-occurring symptoms. That kind of unified treatment gives people more than symptom control. It gives them a better chance at stable, long-term recovery.
How to Start Cognitive Behavioral Therapy in Euless and Dallas
Starting treatment often feels bigger in the mind than it is in real life. Individuals generally do not need to have everything figured out before reaching out. They only need a first step.
For someone in Euless, Dallas, or the surrounding DFW area, the process usually looks something like this:
Make a confidential call
A private conversation can answer basic questions, discuss concerns, and help determine whether treatment is needed now.Complete an assessment
This helps clarify the severity of alcohol use, the presence of mental health symptoms, and whether outpatient care is the right fit.Review insurance and payment options
Many people delay care because they assume treatment will be too complicated or too expensive. Verification often clears up that uncertainty quickly.Begin a personalized plan
The right plan may include PHP, IOP, or standard outpatient therapy, along with dual diagnosis care or medication support when needed.
The important point is this. A person doesn’t have to wait until life falls apart to begin cognitive behavioral therapy for alcohol addiction. Early help can protect jobs, relationships, academic progress, and physical health.
Families can take action too. If a loved one is struggling, the first call can gather information and create a path forward without pressure.
For local support, the next step can start with a confidential call to (888) 385-2051.
Common Questions About CBT for Alcohol Addiction
Some questions tend to come up near the end of the decision-making process. Those questions are normal, especially when a person has tried to stop drinking before.
Frequently Asked Questions About CBT
| Question | Answer |
|---|---|
| Does CBT only work if a person is fully ready to quit? | No. CBT can still help someone who feels ambivalent. It often starts by identifying patterns, triggers, and consequences, which can increase motivation over time. |
| Is CBT just talking about childhood? | No. Past experiences may matter, but CBT usually focuses on current thoughts, behaviors, and practical changes a person can use now. |
| Can CBT help if someone relapsed before? | Yes. CBT is often useful after relapse because it breaks the relapse down into warning signs, thoughts, feelings, and missed opportunities to intervene earlier. |
| Is CBT effective in outpatient treatment? | Yes, and it’s especially useful because clients can practice skills in daily life while still receiving professional support. |
| Can families be involved? | Often, yes. Family involvement can improve communication, reduce enabling patterns, and support a more stable recovery environment. |
| Does CBT replace medication or dual diagnosis care? | Not always. Many people benefit from a combined plan where CBT works alongside medication support and treatment for anxiety, depression, or other co-occurring conditions. |
CBT is practical, not mysterious. It helps people understand why drinking keeps happening and what to do differently when old patterns return. That’s one reason it remains such a trusted approach for alcohol addiction treatment.
Maverick Behavioral Health provides outpatient addiction and mental health treatment for adults in Euless and across the Dallas-Fort Worth area. The program includes CBT-based care at the PHP, IOP, and standard outpatient levels, along with dual diagnosis treatment and medication-assisted treatment when appropriate. To speak with someone confidentially about alcohol addiction treatment, call (888) 385-2051.