

Anxiety is not a simple chemical imbalance, and the old theory behind that idea was debunked by 2011. Anxiety disorders affect over 301 million people globally and 19.1% of U.S. adults in 2021, but there still isn't a blood test or brain scan that can confirm a single chemical deficit as the cause.
That surprises many people because the “chemical imbalance” explanation was repeated for years. It sounded tidy, medical, and reassuring. If one missing brain chemical caused anxiety, then one pill should fix it.
That isn't how anxiety works.
Modern clinical care looks at anxiety as a pattern involving brain communication, stress response, learned coping, environment, and sometimes substance use. That may sound more complicated, but it's better news. A more accurate model gives people more than one path to healing. It opens the door to therapy, nervous system regulation, routine changes, trauma work, medication when appropriate, and integrated treatment for people dealing with both anxiety and addiction in Euless, Dallas, and across the Dallas-Fort Worth area.
Table of Contents
- Anxiety Is Not a Chemical Imbalance But That's Good News
- The Rise and Fall of the Chemical Imbalance Myth
- What Really Happens in an Anxious Brain
- The True Causes of Anxiety A Biopsychosocial View
- The Vicious Cycle of Anxiety and Substance Use
- Effective Anxiety Treatment A Modern Toolkit
- Find Your Path Forward in Dallas-Fort Worth
Anxiety Is Not a Chemical Imbalance But That's Good News
When people search is anxiety a chemical imbalance, they're usually asking two questions at once. What is happening in the brain, and what will help?
The clearest answer is that anxiety isn't a fixed shortage of serotonin, norepinephrine, or another single brain chemical. That model is too narrow. It misses the way anxiety grows out of stress responses, learned patterns, life experiences, physical health, and personal vulnerability.
That's good news because overly simple explanations often lead to overly simple treatment.
Why this shift helps people
If anxiety were only a chemical defect, care would be passive. A person would wait for medication to solve the problem. Medication can help some people, but a fuller understanding gives people more options and more control.
A modern view of anxiety supports treatment that can include:
- Therapy that changes patterns: People can learn how worry loops, avoidance, and catastrophic thinking keep anxiety alive.
- Body-based regulation: Sleep, breathing, movement, and reducing chronic stress can change how the nervous system reacts.
- Trauma-informed care: Past experiences often shape present-day alarm responses.
- Integrated addiction treatment: Alcohol, opioids, stimulants, and sedatives can all complicate anxiety in ways that require coordinated care.
Main takeaway: When the old myth falls apart, treatment gets better. People no longer have to force a complex problem into a one-pill explanation.
What effective care looks like
Good anxiety treatment doesn't ask only, “Which chemical is low?” It asks better questions.
| Better question | Why it matters |
|---|---|
| What triggers the anxiety? | Triggers often reveal patterns that can be changed. |
| What keeps it going? | Avoidance, poor sleep, substances, and chronic stress often maintain symptoms. |
| What else is happening? | Trauma, depression, burnout, and substance use can change the treatment plan. |
| What helps this person function? | Treatment works best when it fits work, family, and daily life. |
That kind of care is more hopeful because it's more accurate. Anxiety is real, physical, and disruptive, but it isn't a sentence to live forever with a broken brain.
The Rise and Fall of the Chemical Imbalance Myth
For a long time, the chemical imbalance story sounded convincing. It said anxiety came from low or faulty neurotransmitters, usually described as serotonin or norepinephrine, and that medication corrected the imbalance.
That message became popular in the late 1980s. It was easy to explain. It was easier to market. And for many people, it reduced shame because it framed anxiety as a medical condition rather than a personal weakness.
Why the theory spread
The theory gave doctors and patients a quick explanation during a period when psychiatric medications were being widely promoted. According to this review of the anxiety chemical imbalance myth, the idea that mental illnesses including anxiety were caused by brain chemical imbalances was popularized from the late 1980s, but by 2011 it had been officially debunked due to a lack of empirical evidence.
A useful analogy is a car with warning lights on the dashboard. Saying anxiety is caused by a chemical imbalance alone is like saying every engine problem comes from low oil. Sometimes oil matters. But wires, sensors, timing, heat, and driver habits matter too. A single-cause explanation feels clean while missing the underlying problem.
Why science moved on
The same review notes that by 2011, Dr. Ronald Pies stated the theory had never been scientifically supported, and drug companies later described it as a “metaphor” rather than a literal explanation. That distinction matters. A metaphor may help people talk about distress, but it shouldn't guide treatment as though it were proven biology.
A metaphor can comfort a patient. It can't replace evidence.
This doesn't mean brain chemistry is irrelevant. It means chemistry isn't the whole story, and it shouldn't be treated like a simple lab value that needs topping off.
What the myth got wrong
The myth failed in three important ways:
- It assumed one-direction causation: Anxiety was framed as the result of a single deficit, instead of a process shaped by stress, behavior, memory, and physiology.
- It encouraged false certainty: People were led to believe a medication corrected a known defect, even though no blood test or scan confirmed that defect.
- It narrowed treatment too much: Many people needed therapy, environmental change, trauma care, or dual diagnosis treatment, not just symptom suppression.
Once that myth is set aside, the conversation becomes more honest. Anxiety can still involve the brain, but the brain works in systems, not slogans.
What Really Happens in an Anxious Brain
An anxious brain isn't broken in one simple place. It's reacting, predicting, scanning, and trying to protect the body.
The better model is a traffic control system. Different brain regions send signals back and forth. Some detect threat. Some weigh context. Some help a person pause, plan, and calm down. Neurotransmitters act more like traffic signals and messengers than fixed “happiness chemicals.”
Anxiety changes brain function in real ways
That doesn't mean anxiety is imaginary. It affects brain chemistry and brain processing. A 2000 1H-MRS study summarized here found that state-trait anxiety significantly altered N-acetyl aspartate (NAA) levels in the orbital frontal cortex, with the strongest effects in males and middle-aged subjects. People in high-anxiety groups showed reduced NAA in that region.
NAA is considered a marker related to neuronal health and function, highlighting its importance. The finding suggests that anxiety can “stress” parts of the brain involved in judgment, emotional evaluation, and response control.
That is very different from saying anxiety is caused by one missing chemical.
Messengers, circuits, and stress response
Several brain chemicals play roles in anxiety:
- GABA: Often associated with calming and inhibition.
- Norepinephrine: Closely tied to alertness and fight-or-flight activation.
- Glutamate: Involved in excitation and learning.
These systems interact with brain circuits that evaluate risk and regulate reactions. When anxiety rises, the brain can start treating ordinary uncertainty like immediate danger. The body then joins in with muscle tension, faster heart rate, shallow breathing, and vigilance.
The key clinical question isn't “Which one chemical is low?” It's “Which alarm systems are getting stuck on?”
Why this matters in treatment
The 1H-MRS findings are useful because they show something nuanced. Anxiety has measurable neurobiological effects, but those changes don't prove a single root cause. They may reflect vulnerability, ongoing stress, or the consequence of repeated anxious activation.
That has practical value in care. Treatment should aim to change the system, not just sedate the symptoms. Therapy can improve interpretation of threat. Routine and sleep can reduce baseline arousal. Medication may support stabilization in some cases. For people with substance use disorders, treatment also has to account for how alcohol or drugs disrupt these same regulatory pathways.
The True Causes of Anxiety A Biopsychosocial View
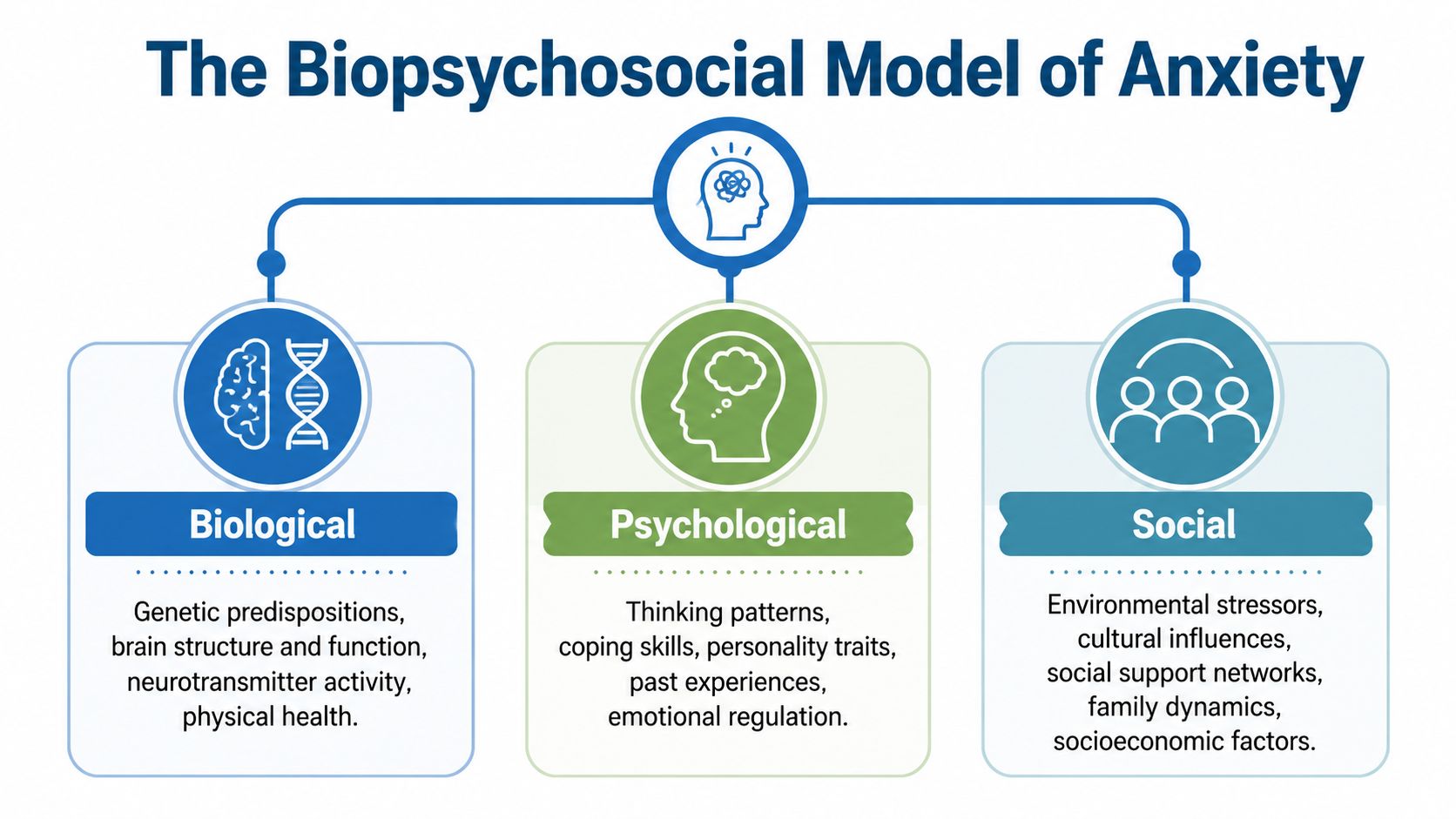
The most useful model for anxiety is biopsychosocial. It doesn't blame one chemical, one event, or one personality trait. It recognizes that anxiety usually develops through the interaction of biology, psychology, and environment.
A person may have inherited sensitivity to stress, learned fear-based coping in childhood, and now live under constant pressure from work, family conflict, or financial strain. None of those factors alone explains the whole picture. Together, they often do.
The three pillars
According to this review of anxiety through a biopsychosocial lens, anxiety emerges from dynamic interactions that include genetic predispositions, environmental stressors, and neuroplastic changes. The same source notes 30 to 50% heritability and that trauma doubles risk with OR=2.1.
Those numbers help clarify what clinicians see every day. Some people arrive with a strong built-in sensitivity. Others develop anxiety after repeated stress, loss, unsafe relationships, or trauma. Many have both.
How the model works in real life
The three parts often look like this:
- Biological influences: Family history, stress reactivity, sleep disruption, physical health, and changes in how the brain adapts to chronic stress.
- Psychological influences: Catastrophic thinking, perfectionism, shame, unresolved trauma, poor emotional regulation, or learned avoidance.
- Social influences: Relationship instability, job strain, isolation, caregiving burden, money stress, or a home environment that never feels safe.
Someone can have strong biology and still get better. Someone can have severe stress and still need help changing learned coping. Both can be true at once.
Why cortisol and threat perception matter
The same source explains that perceived threat can amplify HPA-axis hyperactivity, elevating cortisol and downregulating serotonin receptors without proving a baseline imbalance. That is a more accurate picture of anxiety than the old myth. The brain and body are responding to threat patterns over time.
Treatment should target what is feeding the threat response. If a person has unresolved trauma, insomnia, and constant self-criticism, a prescription alone won't fully address the problem. If a person drinks every night to come down from panic, the anxiety plan has to include substance use treatment too.
A biopsychosocial view doesn't make anxiety more confusing. It makes it more treatable because it gives clinicians and patients a fuller map.
The Vicious Cycle of Anxiety and Substance Use
Many adults don't start using alcohol or drugs because they want to lose control. They start because something works fast. A drink quiets the body. A pill blunts panic. A drug creates relief for a few hours when the nervous system won't settle.
That short-term relief is exactly what makes the cycle dangerous.
Why self-medication backfires
Substances can temporarily lower distress, but they often make the underlying anxiety worse. Sedatives can create rebound anxiety. Alcohol can disrupt sleep and mood regulation. Stimulants can intensify panic, racing thoughts, and physical agitation. Opioids may numb emotional pain, but dependence creates its own fear, instability, and withdrawal cycle.
Over time, the person isn't just treating anxiety anymore. The person is also reacting to cravings, withdrawal, shame, secrecy, and loss of routine.
What dual diagnosis means
When anxiety and substance use are both active, treating only one usually falls short. If a program focuses only on abstinence and ignores panic, trauma, or obsessive worry, relapse risk often stays high. If treatment focuses only on anxiety while ignoring active substance use, the brain and body remain under constant disruption.
That is why integrated care matters. A person needs help with both the anxious system and the addictive pattern at the same time. A closer look at dual diagnosis rehab shows how treatment can be structured around both conditions instead of forcing one to wait.
The cycle clinicians watch for
A common pattern looks like this:
- Anxiety spikes: Stress, intrusive thoughts, trauma reminders, or social pressure increase distress.
- A substance brings relief: The person feels calmer, detached, or more able to function.
- The rebound arrives: Sleep worsens, mood drops, or the nervous system becomes more reactive.
- Use becomes the coping plan: The person starts needing the substance not to feel good, but to avoid feeling worse.
When anxiety and addiction are linked, “just stop using” isn't a complete treatment plan. The fear system also has to be treated.
In Euless, Dallas, and the larger DFW area, this is one of the most common reasons outpatient care needs to be individualized. Working adults often hide both problems well. The suffering is real anyway.
Effective Anxiety Treatment A Modern Toolkit
If anxiety isn't a chemical imbalance, treatment has to do more than chase one chemical. It needs to help the brain and body become more flexible, less reactive, and better able to recover from stress.
The most effective plans usually combine several tools instead of relying on a single answer.
What works better than a one-track approach
Emerging neuroimaging findings summarized in this review of anxiety-related chemical variation link anxiety to variations in NAA, GABA, and glutamate by sex and age. The same review notes that these findings do not support an imbalance-causation theory, but they can help point toward individualized strategies, including exercise, therapy, and other non-medication approaches that support regulation.
That principle matters in practice. Different people need different combinations.
- Psychotherapy: Skills-based therapy helps people identify distorted thinking, reduce avoidance, process trauma, and build tolerance for uncertainty. For many adults, structured work such as cognitive behavioral therapy for addiction recovery also helps when alcohol use has become part of the anxiety pattern.
- Medication when appropriate: Medication can reduce symptom intensity enough for a person to engage in therapy and daily life. It works best as one tool within a broader plan, not as proof that a broken chemical has been corrected.
- Somatic and lifestyle supports: Exercise, sleep stabilization, breath work, routine, and group support can help calm the stress response without adding the risks that come with overreliance on sedating substances.
Where MAT fits
For people with co-occurring opioid use, Medication-Assisted Treatment can be a critical part of stabilization. MAT doesn't “cure” anxiety, but it can reduce withdrawal and cravings so the person can participate in therapy and rebuild daily functioning.
One outpatient option in the DFW area is Maverick Behavioral Health, which provides PHP, IOP, dual diagnosis care, and MAT including Suboxone. In a practical treatment plan, that kind of structure can help a person address opioid dependence and anxiety at the same time rather than treating them as separate crises.
A practical treatment lens
A strong anxiety plan asks:
| Treatment tool | What it targets |
|---|---|
| Therapy | Thoughts, behaviors, trauma responses, avoidance |
| Medication | Symptom relief and stabilization when clinically appropriate |
| MAT | Cravings and withdrawal in co-occurring opioid use |
| Holistic supports | Stress physiology, routine, sleep, body regulation |
The goal isn't perfection. The goal is steadier function, fewer fear-driven behaviors, and a life that no longer revolves around managing symptoms hour by hour.
Find Your Path Forward in Dallas-Fort Worth
Learning that anxiety isn't a simple chemical imbalance can feel unsettling at first. Then it often becomes a relief. It means the struggle isn't about one missing substance in the brain that a person is powerless to change.
It means there are multiple points where healing can begin.
What outpatient help can look like
For many adults in Euless, Dallas, and the greater Dallas-Fort Worth area, outpatient treatment makes practical sense. Some need more support than a weekly therapy session but don't need inpatient care. Others are balancing work, family, or school and need a schedule that fits real life.
Programs such as PHP and IOP can offer that middle ground. They create enough structure for meaningful progress while allowing people to stay connected to daily responsibilities.
Who should consider a higher level of support
A stronger treatment setting may be worth considering when any of these are true:
- Anxiety is disrupting basic life: Work, sleep, parenting, concentration, or relationships are falling apart.
- Substances have become part of coping: Alcohol, pills, opioids, or stimulants are being used to calm down, get through the day, or avoid withdrawal.
- Past treatment hasn't been enough: Brief counseling or medication alone hasn't addressed the full picture.
- Trauma or co-occurring symptoms are present: Panic, depression, substance use, and chronic stress often need integrated care.
The right level of care should match the level of disruption, not the level of pride.
Taking the first step
People often wait too long because they think they should be able to push through. Anxiety rarely responds well to white-knuckling. What helps is an accurate assessment, a treatment plan that fits the person, and enough support to follow through.
For someone preparing to start care, how to prepare for a first therapy session can make the first appointment feel less overwhelming and more productive.
Recovery in DFW doesn't have to start with certainty. It can start with a conversation, a screening, or one honest admission that the current pattern isn't working. That is often the turning point.
If anxiety, alcohol use, drug use, or all of them together are affecting daily life, Maverick Behavioral Health offers outpatient mental health and substance use treatment for adults in Euless, Dallas, and across the DFW area. PHP, IOP, dual diagnosis care, and MAT can be personalized for the individual rather than forced into a one-size-fits-all model. Call (888) 385-2051 to speak with a compassionate team member about next steps.