


A lot of families in Dallas-Fort Worth start the same way. It’s late, someone is spiraling, and a spouse, parent, or adult child is searching for help with one urgent question in mind. Can they find treatment that’s affordable and fast enough to matter right now?
That’s where state funded drug rehab in texas often enters the picture. It’s a real option, and for many people it’s an important one. But it’s rarely as simple as finding a bed, filling out one form, and starting care the next day. The system can help. It can also feel slow, fragmented, and hard to work through when a person is in immediate danger of relapsing, overdosing, losing housing, or walking away from treatment altogether.
Table of Contents
- The Search for Hope and Help in North Texas
- What State-Funded Rehab in Texas Really Means
- How to Find and Apply for State Treatment Programs
- Navigating the Reality of Waitlists and Access Gaps
- The Critical Role of MAT and Dual Diagnosis Care
- Effective Alternatives When You Cannot Afford to Wait
- Frequently Asked Questions About Texas Rehab Funding
- Is state-funded rehab completely free
- What if someone has insurance but can’t afford high out-of-pocket costs
- Can someone work while getting treatment
- What if the person is denied state-funded treatment
- Can courts be involved in treatment access
- What’s the most important factor when choosing between waiting and starting elsewhere
The Search for Hope and Help in North Texas
In Euless, Dallas, Fort Worth, and the surrounding metro area, the search usually starts in a rush. A family may have just found fentanyl, pills, or empty bottles. An employer may have issued one last warning. A person may be asking for help for the first time, and everyone knows that window can close fast if the process drags on.

State-funded treatment exists for exactly these moments. It was built to give people a path to care when private payment isn’t realistic and insurance coverage is limited or absent. That matters in a state where need is high and access is uneven.
According to Texas treatment access data reported by KVIA, Texas ranked #51 in the U.S. in 2021 for the share of its population receiving substance use treatment, with only 116 people per 100,000 residents in care, despite having over 500 treatment facilities and 14.8% of the population affected by a substance use disorder.
That gap is why the search feels so frustrating. People assume that if treatment programs exist, treatment must be available. In practice, families often find a maze of screenings, eligibility rules, referrals, and waiting periods. The system isn’t useless. It’s just under strain.
What families usually need in the first 24 hours
Some families need detox guidance. Others need outpatient support that can start quickly so a person can keep working, parenting, or attending school while stabilizing. Many just need someone to explain the next move in plain language.
Common priorities include:
- Speed: The person is willing today, and the family doesn’t want to lose momentum.
- Affordability: Cost may be the first barrier discussed at home.
- Local access: Transportation across DFW can become a treatment barrier fast.
- A realistic level of care: Not everyone needs the same setting.
For readers who need local options in Dallas County, this guide to drug rehab in Dallas may help clarify what outpatient treatment can look like close to home.
A family doesn’t need a perfect plan on day one. It needs a safe next step.
What State-Funded Rehab in Texas Really Means
State-funded rehab generally refers to substance use treatment supported by public funding and administered through Texas systems that serve residents who can’t easily access private care. These programs are designed to expand treatment access, especially for people with low income, limited resources, no insurance, or major clinical need.
That doesn’t mean every program is identical. Some offer withdrawal support, some focus on residential care, and others provide outpatient services or referral-based placement. The exact pathway depends on clinical need, local availability, and whether the person meets financial and residency criteria.

What these programs are meant to do
The public system is built to serve people who might otherwise go untreated. In plain terms, it tries to answer a hard question. If someone needs addiction care but can’t afford standard private treatment, where can that person go?
Programs commonly aim to provide:
- Assessment and triage: Determining whether a person needs detox, residential treatment, outpatient care, or referral elsewhere.
- Core treatment services: Counseling, recovery planning, relapse prevention, and case coordination.
- Access routes for uninsured residents: A public entry point for people who don’t know where to begin.
- Connection to ongoing care: Moving people from crisis toward a longer-term recovery plan.
Who usually qualifies
Eligibility is often based on practical criteria rather than a single simple checklist. Programs may ask for proof of Texas residency, income information, insurance status, and clinical information about substance use severity. Some people assume they won’t qualify and never call. Others assume they’ll be admitted immediately and get blindsided by the screening process.
A stronger approach is to gather the paperwork early and expect questions about:
- Residency in Texas
- Income and household situation
- Current insurance or lack of coverage
- Substance use history
- Immediate safety concerns
- Mental health symptoms or psychiatric history
People who aren’t sure whether private insurance could help should check benefits before assuming the only option is public funding. This overview of how insurance verification works for treatment can help families understand that process.
Why access still matters so much
Public treatment isn’t just an administrative issue. It’s a safety issue. According to Texas overdose data summarized here, 4,416 people lost their lives to overdose between August 2023 and July 2024, even though overdose deaths had declined from the prior period. The same source notes that successful completion of a treatment program can lead to a 40-60% chance of recovery or significantly reduced use.
Practical rule: If a person is at immediate risk, the best treatment option is the one that can start safely and quickly.
What state-funded care does well and where it gets hard
State-funded care can be life-saving. It gives many Texans access they would not otherwise have. It can also be uneven in availability, narrow in service offerings, and slower than families expect.
The biggest mistake is treating the phrase “state-funded rehab” as if it refers to one standard program. It doesn’t. It refers to a network with different providers, different wait times, different treatment models, and different admission thresholds. Families usually do better when they ask detailed questions instead of assuming every publicly funded option offers the same level of care.
How to Find and Apply for State Treatment Programs
Once a family decides to pursue state funded drug rehab in texas, the next challenge is dealing with the intake process without getting discouraged. The system becomes easier to handle when it’s broken into practical actions rather than vague advice.
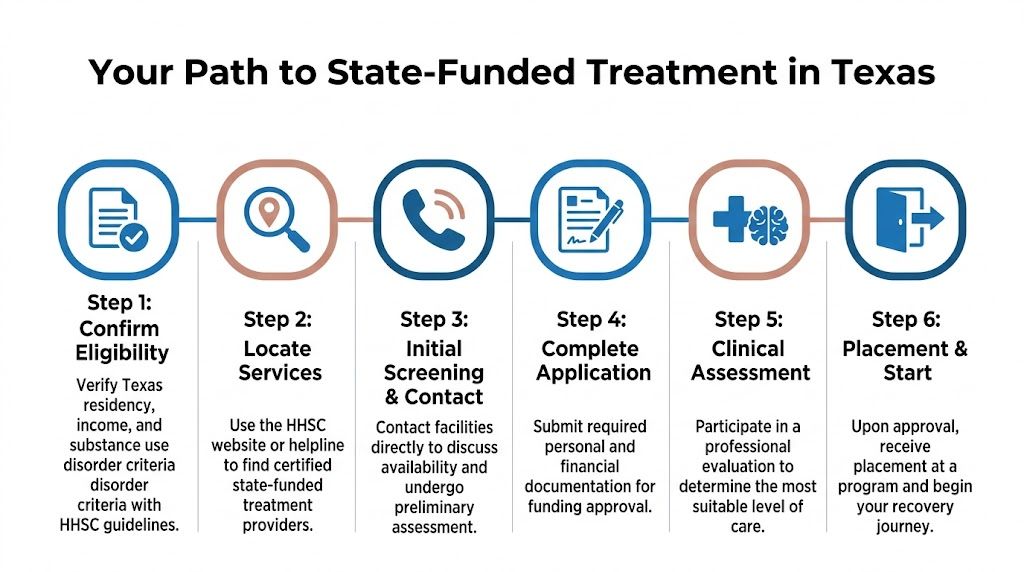
Start with the correct local entry point
Individuals rarely enter public treatment by calling random facilities one by one. They usually need to connect with the appropriate local behavioral health access point or a treatment referral source that can direct screening and placement.
That first contact matters because it shapes everything that follows. If the person reaches the wrong office, gives incomplete information, or waits days to return a call, the process can stall before an assessment even happens.
A productive first call usually covers:
- Current substance use: What’s being used, how often, and whether withdrawal is a concern.
- Safety issues: Overdose history, suicidal thinking, unstable housing, or acute psychiatric symptoms.
- Basic eligibility details: Texas residency, insurance status, and income concerns.
- Location logistics: Whether the person can realistically travel across DFW for care.
Expect screening before placement
Families often ask for a bed or an appointment right away. Public systems usually start with a screening instead. That screening is not pointless bureaucracy. It’s how the system decides what level of care is clinically appropriate.
The questions may feel repetitive. They still matter. A person may need detox before outpatient treatment. Another may need dual diagnosis support because untreated depression, trauma, or anxiety is driving substance use. Someone else may be stable enough for structured outpatient care if it can begin quickly.
Gather documents before anyone asks twice
Delays often happen because the clinical side moves faster than the paperwork side. Families can reduce frustration by preparing the common documents before the process reaches that stage.
Useful documents often include:
- Photo identification
- Proof of Texas residency
- Income or unemployment information
- Insurance cards if any coverage exists
- Medication list
- Discharge papers from ER visits, detox, or prior treatment
- Contact information for emergency supports
A family doesn’t always need every item in hand on the first call. But having them ready prevents a common problem. The person gets motivated, starts the process, then disappears once paperwork requests pile up.
The practical goal isn’t to complete the process perfectly. It’s to keep the person engaged long enough to reach the first real treatment appointment.
Be ready for a level-of-care decision that may not match expectations
Some people expect residential treatment and are referred to outpatient. Others want something flexible and learn they first need medical stabilization. That mismatch can trigger resistance if nobody prepared the family for it.
A helpful way to think about the assessment is this. It’s not deciding who deserves help. It’s deciding what type of help fits the person’s current condition.
Here are the questions families should ask after the assessment:
- What level of care is being recommended right now?
- Is there a wait for that level of care?
- What should the person do while waiting?
- If that placement isn’t available soon, what is the backup plan?
- Does the referral include mental health services if needed?
Follow-up is part of the application
Many admissions fall apart after the first conversation. A voicemail goes unanswered. A document doesn’t get sent. A person misses an intake window by a day or two and the family assumes the opportunity is gone.
That’s why follow-up matters as much as the initial call.
A family should keep a simple written record with:
| Item | What to track |
|---|---|
| Contact name | The person or office spoken to |
| Date | When the call or email happened |
| Next action | What must be submitted or completed |
| Deadline | When the person needs to respond |
| Backup contact | Another route if the first person doesn’t answer |
If the process slows down
A stalled application doesn’t always mean denial. It may mean the program is full, the person needs another screening, or paperwork is incomplete. Families should call back, ask direct questions, and request the next action in plain language.
That includes asking whether there are interim options. Even when state-funded placement takes time, some people can begin support elsewhere while waiting. That might include outpatient counseling, medication support, recovery meetings, family support, or a private program that can stabilize the situation before a public opening becomes available.
Navigating the Reality of Waitlists and Access Gaps
The biggest misunderstanding about state funded drug rehab in texas is that approval automatically means timely treatment. For many people in North Texas, it doesn’t. They may qualify, complete screening, and still wait longer than is clinically safe.

According to analysis of Texas state-funded treatment access, waitlists often exceed 30-60 days, and DFW metro areas have over 20% fewer beds per capita compared to rural areas. The same analysis notes a 15% rise in opioid-related admissions, which puts even more pressure on already limited capacity.
Why DFW feels especially tight
Dallas-Fort Worth combines high demand, transportation barriers, population density, and a large number of people trying to hold together work and family responsibilities while seeking care. A person may technically be offered treatment, but not at a location, schedule, or start date that’s workable.
That creates a dangerous gap between eligibility and actual treatment entry. Motivation drops. Withdrawal gets worse. Family support burns out. Some people return to use because there’s no immediate structure in place.
What families can do while waiting
Waiting doesn’t have to mean doing nothing. The strongest approach is to treat the waitlist period as active risk management.
Useful actions include:
- Keep daily contact with the referral source: Ask whether cancellations or earlier openings exist.
- Clarify the safety plan: Know what to do if the person relapses, threatens self-harm, or experiences severe withdrawal.
- Use interim support: Outpatient counseling, medication support, family involvement, and recovery meetings can help hold the line.
- Document changes: If symptoms worsen, report that quickly. A new clinical picture can affect placement decisions.
A waitlist is not neutral time. For someone with active addiction, every unstructured week carries risk.
If the person is denied or deprioritized
Denial doesn’t always mean the person has no options. Sometimes it means the program believes a different level of care fits better, the documentation is incomplete, or another system should handle the case first. Families should ask for the reason in plain language and ask what referral path is being recommended instead.
Questions worth asking include:
- Was the denial financial, clinical, or administrative?
- Can the person reapply with updated information?
- Is there an appeals process or review option?
- What care is recommended right now instead of waiting with no support?
Some families make the mistake of reading “not admitted” as “not serious enough” or “not wanted.” It often just means the public system has limits the family now has to work around.
The Critical Role of MAT and Dual Diagnosis Care
A treatment slot isn’t enough if the program can’t address the actual drivers of relapse. Two of the most important pieces of modern addiction care are Medication-Assisted Treatment (MAT) and dual diagnosis treatment for co-occurring mental health conditions.
MAT matters because cravings, withdrawal, and physiological dependence can overpower good intentions. For opioid use disorder, medications such as Suboxone can reduce withdrawal symptoms and cravings so a person can engage in counseling and daily life more consistently. Without that support, many people drop out early or return to use before therapy has time to help.
Dual diagnosis care matters for a different reason. A large number of people don’t just have a substance problem. They also have depression, anxiety, trauma symptoms, bipolar disorder, panic, grief, or other psychiatric concerns that feed the cycle. If treatment addresses substance use but ignores mental health, progress often stalls.
Why this gap changes outcomes
Families sometimes assume all rehab programs offer these services. They don’t. According to Texas provider details on treatment access, despite over half of individuals with substance use disorders also having a co-occurring mental health condition, only about 35% of Texas state-funded rehabs offer MAT.
That gap matters most for people facing opioid dependence, repeated relapse, or unstable psychiatric symptoms. A person may enter a program willing to work, only to find the treatment model doesn’t include the medication support or integrated mental health care that would make sustained engagement realistic.
What to ask before accepting placement
Before a family commits to any program, it helps to ask direct treatment-quality questions rather than focusing only on admission.
Key questions include:
- Does the program offer MAT on site or through a coordinated referral?
- Can the person continue prescribed medication if already stable on it?
- Are mental health and addiction treated together, or separately?
- Who manages psychiatric symptoms during recovery?
- What happens after discharge?
A program doesn’t have to be perfect. It does need to fit the person’s risks.
What strong outpatient support looks like
For many adults in DFW, the most practical model is outpatient care that combines therapy, structure, medication support, and continued family involvement. That’s especially true when the person can’t step away from work, parenting, or school for a long residential stay.
Families looking into medication support can review how a MAT program works in outpatient treatment and what questions to ask about continuity, safety, and follow-up care.
Good addiction treatment doesn’t separate the mind from the substance problem. It treats both at the same time.
Effective Alternatives When You Cannot Afford to Wait
When state placement is delayed, the family still has to answer the same question. What helps right now?
The best answer is often a practical one, not an ideological one. If immediate public placement isn’t available, a person may do better starting with a flexible outpatient program, medication support, family coordination, and a schedule they can sustain. Fast entry matters because treatment engagement is fragile at the beginning.
According to completion and recovery data on addiction treatment, less than 43% of individuals complete addiction treatment, while those who do complete treatment have a 40-60% success rate. That makes delays costly. Long waits can increase dropout risk before treatment even begins.
What often works better than waiting passively
Not everyone needs the same solution, but a few alternatives are often worth exploring right away:
- Immediate outpatient treatment: This can provide structure, therapy, and accountability while the person stays at home.
- Partial hospitalization or intensive outpatient care: These models can offer more support than standard weekly counseling without the disruption of full residential placement.
- Medication support for opioid or alcohol use disorders: This can reduce cravings and help a person stabilize quickly.
- Private care with insurance verification: Many families assume private outpatient treatment is out of reach when it may be more feasible than expected.
- Bridge planning: Some people use outpatient treatment now and reassess public placement later if a higher level of care is still needed.
Why outpatient care fits many DFW adults
For working professionals, parents, college students, and adults with basic stability at home, outpatient treatment can solve a problem state systems often can’t solve quickly. It allows care to begin without waiting for a residential opening, and it can be built around real life instead of requiring life to stop first.
That flexibility matters in North Texas, where distance, job schedules, and child-care responsibilities are often part of the clinical picture. A treatment plan only works if the person can attend it.
Comparing treatment paths
| Factor | State-Funded Programs | Maverick Behavioral Health (Private Outpatient) |
|---|---|---|
| Entry timing | May involve screening, referral, and waitlist delays | Can offer a faster path to admissions review and scheduling |
| Flexibility | Varies by program and placement availability | Designed for outpatient scheduling, including IOP and PHP |
| MAT access | Not available at every public program | MAT is part of the outpatient treatment model |
| Dual diagnosis support | Can be limited or fragmented depending on placement | Integrated substance use and mental health treatment |
| Fit for work and family life | May depend on the assigned level of care | Built for adults who need structured care without full residential disruption |
| Continuity | Can depend on referral handoffs | Ongoing outpatient planning and aftercare support |
When a private outpatient option makes sense
A private outpatient center is often the better fit when:
- The person is willing now and may not stay willing for weeks
- The family needs evening or daytime structure without a residential stay
- Opioid use requires rapid MAT access
- Mental health symptoms are part of the addiction pattern
- The person needs a discreet local option in the Euless or Dallas area
The key trade-off is straightforward. Public care may reduce direct cost but can come with delay and narrower service availability. Private outpatient care may offer faster access, stronger scheduling flexibility, and more consistent MAT or dual diagnosis support. For many families, that speed is what protects the person long enough for recovery to take hold.
Frequently Asked Questions About Texas Rehab Funding
Is state-funded rehab completely free
Sometimes, but not always in the way families expect. Publicly funded treatment is meant to reduce financial barriers, but eligibility rules, documentation requirements, and provider availability still shape what a person can access. Some programs may be fully covered for eligible residents, while others may involve limited slots, referral requirements, or related costs outside the main treatment episode.
What if someone has insurance but can’t afford high out-of-pocket costs
That person shouldn’t assume public care is the only option. Insurance verification can reveal outpatient benefits that make treatment much more manageable than expected. A family should ask what level of care is covered, whether prior authorization is needed, and whether medication support and mental health treatment are included.
Can someone work while getting treatment
Often yes, especially in outpatient models. Many adults in DFW need care that fits around jobs, parenting, or school. That’s one reason flexible outpatient treatment is often a practical solution when full residential treatment isn’t necessary or available.
What if the person is denied state-funded treatment
The family should ask why. Denials can be clinical, administrative, or based on incomplete information. The next question should always be, “What care should start now?” Even if a public program says no, the person may still qualify for another level of care, a different referral route, or an outpatient bridge option.
Can courts be involved in treatment access
Yes, sometimes. A court-related referral may affect how quickly someone is assessed or what documentation is required. Even then, the person still needs a clinically appropriate placement and a realistic continuing-care plan. A legal referral doesn’t automatically solve access problems or guarantee the right services.
What’s the most important factor when choosing between waiting and starting elsewhere
The safest choice is usually the one that keeps the person engaged in care now. If motivation is fragile, relapse risk is high, or opioid use is involved, delay can be dangerous. Families should weigh cost, timing, treatment quality, MAT availability, and mental health support together instead of focusing on just one factor.
Families in Euless, Dallas, and across DFW don’t have to sort through this alone. Maverick Behavioral Health provides outpatient addiction and mental health treatment with flexible IOP and PHP options, dual diagnosis support, and MAT including Suboxone. For immediate guidance on treatment options and insurance verification, call (888) 385-2051.