

Some people in Euless, Dallas, and the surrounding DFW area start searching for help late at night. They may be exhausted, scared of withdrawal, and unsure whether treatment will work this time. They may have promised themselves or their family that they’d stop, only to find that cravings and sickness took over again.
That moment matters. It often means a person isn't looking for a lecture. They’re looking for something that can help them get stable, breathe, and think clearly enough to start rebuilding life.
What is medication assisted treatment? In plain language, it’s a medical approach that uses prescribed medication together with counseling and behavioral support to treat substance use disorders, especially opioid use disorder. It isn’t a shortcut, and it isn’t giving up. It’s treatment that addresses both the body and the mind.
Table of Contents
- Finding a Lifeline When You Feel Trapped by Addiction
- How MAT Restores Balance to Your Brain and Life
- A Closer Look at Common MAT Medications
- MAT Is More Than Just Medication
- Your First Steps with MAT at Maverick Behavioral Health
- Addressing Common Myths and Concerns about MAT
- Frequently Asked Questions About Starting MAT in Dallas
- How long will someone stay on MAT medication
- Can someone still work or go to school while receiving MAT
- Does insurance cover MAT
- What if the person also has anxiety, depression, or another mental health concern
- What is the first step to get started in Dallas or Euless
- What should a family member do if they’re the one reading this
Finding a Lifeline When You Feel Trapped by Addiction
A person may wake up feeling sick, promise not to use again, make it through a few hard hours, and then use to stop the crash. By evening, shame sets in. The next day, the same cycle repeats.
That pattern can make people believe they’re weak. They aren’t. Opioid addiction changes how the brain and body function, which is one reason quitting can feel impossible without medical support.
Medication-assisted treatment, often called MAT, gives people a safer and more stable path into recovery. It combines FDA-approved medication with counseling and behavioral therapies. The medication helps with cravings and withdrawal. Therapy helps people repair routines, relationships, and decision-making.
Many patients feel relief when they learn that MAT isn't a moral compromise. It's a medical response to a medical condition.
For people asking what is medication assisted treatment, the simplest answer is this: it helps the body settle down so recovery work can begin.
That matters because opioid use disorder is widespread, and treatment still doesn’t reach everyone who needs it. In 2023, 2.3 million Americans received medication-assisted treatment for opioid use disorder, yet nearly 54.2 million people needed substance abuse treatment overall. That gap shows why MAT remains a critical and underused standard of care, as reported by drug abuse treatment data on MAT access.
Why people often look for MAT
Some people consider MAT after a relapse. Others look into it after trying to quit on their own and finding that withdrawal drove them back to use. In outpatient settings around Dallas-Fort Worth, people also ask about MAT because they need treatment that fits real life.
- Work still matters: Many adults need to keep showing up for a job while getting help.
- Family responsibilities don’t pause: Parents still need to handle school pickups, meals, and home life.
- Privacy matters: Plenty of people want care that feels confidential and structured, not chaotic.
- Fear of withdrawal is real: For many, that fear is the biggest barrier to making the first call.
MAT doesn't erase the need for effort. It gives that effort a real chance to work.
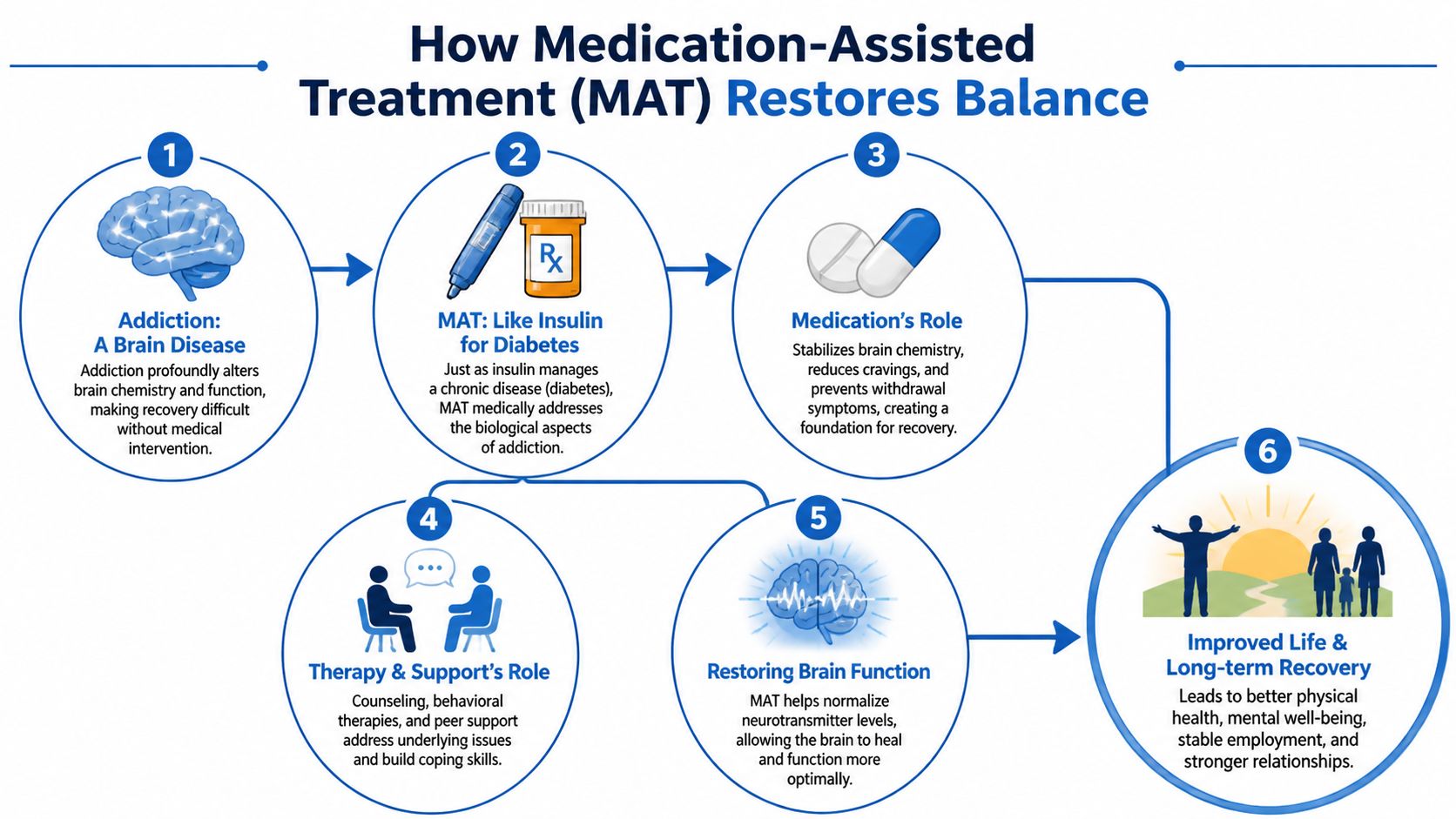
How MAT Restores Balance to Your Brain and Life
A helpful way to understand MAT is to compare it to insulin for diabetes. Insulin doesn’t cure diabetes, but it helps the body function more normally so the person can live, work, and take care of themselves. MAT works in a similar way for opioid use disorder. It treats the biological part of the illness so a person can participate in recovery.
Why willpower alone often isn’t enough
Repeated opioid use changes the brain systems involved in reward, stress, and survival. That’s why a person can want to stop and still feel pulled back toward use. Cravings can become loud. Withdrawal can feel overwhelming. Daily judgment gets narrower and more urgent.
When families don’t understand that biology, they sometimes say things like, “Why can’t they just stop?” The better question is, “What support will help the brain and body stabilize enough for recovery to take hold?”
Practical rule: When a treatment reduces withdrawal and cravings, it creates room for therapy, structure, and healthier choices to start working.
MAT is important because it helps lower that level of internal chaos. According to Pew’s MAT fact sheet on opioid use disorder outcomes, MAT is the most effective intervention for opioid use disorder, reducing illicit opioid use by up to 50% more than therapies alone and cutting overdose fatalities in half.
What the medication actually does
The medication side of MAT doesn’t “fix” a person overnight. What it often does is much more practical.
- Reduces withdrawal symptoms: Instead of feeling physically hijacked, the person can get through the day with less distress.
- Lowers cravings: The mind isn’t constantly pulled toward using.
- Supports steadier thinking: A calmer nervous system makes it easier to attend therapy and follow a plan.
- Creates a foundation for routine: Sleep, meals, work, appointments, and family time become more manageable.
The “assisted” part matters too. Medication handles part of the biological problem. Counseling and recovery support help people learn how to respond to stress, avoid old patterns, rebuild trust, and cope without substances.
A simple example helps. If someone is spending most of the day trying not to get sick, they won’t have much energy left for group therapy, parenting, or problem-solving. If medication eases that physical battle, the person can finally focus on the deeper work.
That’s why MAT is often less about replacing one thing with another and more about restoring enough balance for recovery to become possible.
A Closer Look at Common MAT Medications
People often hear the term MAT and assume it means one medication. It doesn’t. Several medications can be used, and each works a little differently. The right fit depends on a person’s opioid use history, withdrawal pattern, treatment goals, daily schedule, and medical needs.
Buprenorphine and Suboxone
Buprenorphine is a common MAT medication in outpatient care. Many patients know it by the brand name Suboxone, which combines buprenorphine with naloxone. Buprenorphine attaches strongly to opioid receptors but works as a partial agonist, which means it can reduce cravings and withdrawal without producing the same effect as full opioids.
That partial action is important. Buprenorphine creates a ceiling effect that lowers overdose risk, and it has been associated with a 55% reduction in serious opioid-related acute care needs at 12 months compared with no treatment, according to CDC-linked guidance on buprenorphine treatment.
For many people in outpatient treatment, Suboxone feels less like a dramatic change and more like relief. They often describe feeling more normal, less panicked, and better able to think. A fuller overview of this approach appears in Maverick’s guide to medication-assisted treatment for opioid addiction.
Methadone and naltrexone
Methadone is a full opioid agonist used in structured treatment settings. It can help people who need a medication with strong withdrawal and craving control. For some patients, that structure is useful and appropriate.
Naltrexone works differently. It blocks opioid effects rather than activating opioid receptors. That makes it a very different experience from buprenorphine or methadone. It may fit people who have already completed detox and want a blocking medication as part of relapse prevention.
The “best” medication is the one that matches the person’s clinical needs, daily life, and ability to stay engaged in treatment.
MAT medications at a glance
| Medication | How It Works | Best For | Form |
|---|---|---|---|
| Buprenorphine or Suboxone | Partially activates opioid receptors to reduce cravings and withdrawal with a ceiling effect | Many outpatient patients who need flexibility and symptom relief | Commonly taken as an oral or sublingual medication |
| Methadone | Fully activates opioid receptors in a controlled treatment setting to prevent withdrawal and reduce cravings | People who need a highly structured approach | Taken as a prescribed medication through regulated care |
| Naltrexone | Blocks opioid effects rather than activating receptors | People who have already detoxed and want a blocking medication | Available in prescribed formulations including injection options |
Patients don’t need to pick a medication on their own before calling a program. The point is to understand that there are options, and a clinician can help sort through them.
MAT Is More Than Just Medication
One reason MAT gets misunderstood is that people focus only on the prescription. But medication is only one part of the treatment plan. It helps steady the body. It doesn’t automatically teach someone how to handle grief, relationship conflict, anger, boredom, shame, or trauma.

Why therapy matters so much
Once cravings and withdrawal become more manageable, therapy starts to matter in a different way. Patients can pay attention. They can remember what they discussed. They can notice triggers instead of reacting to them automatically.
Treatment usually needs to address questions like these:
- What happens right before use? Some people use after conflict. Others use when they feel alone, ashamed, or overstimulated.
- What has addiction disrupted? Work habits, sleep, family trust, nutrition, and mental health often need repair.
- Which skills are missing? Many people need help with emotional regulation, boundaries, or relapse prevention planning.
- What support will continue outside sessions? Recovery works better when people build a real support network.
Group therapy can be especially helpful because it reduces isolation. People hear their own fears in someone else’s words. Families also benefit when they learn that recovery is a process, not a single decision.
What support can look like in outpatient care
Outpatient MAT often works best when it’s part of a broader plan such as individual counseling, group therapy, and structured programming. Some patients need a more intensive schedule at first. Others need a level of care that lets them keep working or attending school.
For people who also benefit from community support, virtual Narcotics Anonymous meeting options can be one way to add connection outside formal treatment hours.
Medication can quiet the noise. Therapy helps a person understand what the noise was covering up.
A strong treatment plan usually combines medical monitoring with practical recovery work. That may include managing triggers, repairing daily habits, addressing mental health symptoms, and preparing for high-risk moments before they happen. MAT supports that process, but it doesn’t replace it.
Your First Steps with MAT at Maverick Behavioral Health
For many people, the hardest part is not taking medication. It’s not knowing what to expect. Uncertainty makes treatment feel bigger and scarier than it is.

What happens before the first dose
At an outpatient center such as Maverick Behavioral Health’s MAT program in the DFW area, the process often starts with a confidential phone call and an assessment. The team asks about substance use, health history, current symptoms, mental health needs, and practical concerns such as work, transportation, and schedule.
That first conversation usually helps answer questions like:
- Is MAT appropriate for this person?
- Which medication might fit best?
- What level of care makes sense right now?
- Are there co-occurring mental health concerns that need attention too?
If buprenorphine is the medication plan, timing matters. A proper induction protocol involves confirming mild withdrawal, often measured with a COWS score of 4 to 12, before starting buprenorphine so that precipitated withdrawal is avoided. According to American Addiction Centers’ MAT medication overview, this kind of precise induction is associated with strong retention, with some practices reporting 80% of patients remaining in treatment at 6 months.
What day one and early follow-up can feel like
Patients often expect day one to feel dramatic. In reality, it’s usually careful and clinical. The goal is to start safely, monitor symptoms, and adjust thoughtfully.
A typical early experience may include:
- Assessment and orientation: Staff explain the treatment plan, answer questions, and discuss what symptoms to watch for.
- Medication start: The first dose is given only when the timing is right for that medication.
- Observation and feedback: The patient reports how they feel, and the clinician adjusts if needed.
- Follow-up visits: Early appointments help fine-tune the dose and support stability.
Some people feel relief quickly. Others need adjustments and patience. Neither response means treatment is failing. Early stabilization is a process.
Early MAT should feel organized, monitored, and collaborative. Patients shouldn't have to guess what comes next.
For residents of Euless and Dallas, this step-by-step approach often lowers fear. A clear plan makes it easier to say yes to treatment.
Addressing Common Myths and Concerns about MAT
MAT still carries a lot of stigma, and that stigma stops people from getting help. Some patients worry about what family members will think. Others fear they’ll be judged at work, in recovery circles, or even by people who care about them.
The most common fear
The biggest myth is that MAT is “just trading one drug for another.” That idea sounds simple, but it misses the difference between compulsive, harmful substance use and a prescribed, monitored treatment plan.
A person actively addicted to opioids is usually chasing relief, avoiding withdrawal, and living with instability. A person on MAT is using medication in a structured medical setting to reduce cravings, improve functioning, and support recovery. Those are not the same thing.
Stigma remains a serious barrier. According to SMART Recovery’s discussion of stigma and MAT, only 5% of people with opioid use disorder receive MAT, in part because of the misconception that it substitutes one addiction for another, even though MAT is associated with a 50% boost in survival rates.
Other questions families often ask
Families also ask whether MAT is safe, whether it changes personality, and whether being on medication means a person isn’t “really sober.” Those concerns usually come from fear, not bad intent.
A few grounded answers help:
- Safety depends on proper medical care: MAT should be prescribed and monitored by qualified clinicians.
- Medication isn't the whole recovery story: A person still needs counseling, structure, and accountability.
- Recovery doesn’t have to look the same for everyone: What matters is stability, honesty, health, and reduced risk.
- Longer treatment isn't failure: Some people need more time on medication, and that can be part of responsible care.
People deserve treatment based on evidence and fit, not shame.
Frequently Asked Questions About Starting MAT in Dallas
How long will someone stay on MAT medication
There isn’t one timeline that fits everyone. Some people need medication for a shorter period, while others benefit from staying on it longer. The decision should be based on stability, relapse risk, daily functioning, and medical guidance, not pressure or stigma.
Can someone still work or go to school while receiving MAT
Often, yes. Outpatient MAT is commonly chosen because it can fit around work, school, and family responsibilities. The care team usually helps build a schedule that supports treatment while protecting daily obligations as much as possible.
Does insurance cover MAT
Coverage depends on the person’s plan and the services involved. Many outpatient programs help verify benefits and explain options before admission, which can reduce some of the stress around getting started.
What if the person also has anxiety, depression, or another mental health concern
That’s common. Many people need treatment that addresses both substance use and mental health at the same time. When both are treated together, recovery planning becomes more realistic and more useful.
What is the first step to get started in Dallas or Euless
The first step is a confidential call to discuss symptoms, substance use, safety, and scheduling. That call can help determine whether MAT is appropriate and what the next appointment should look like.
What should a family member do if they’re the one reading this
A family member can call too. They can ask questions, learn what MAT is, and find out how to support a loved one without judgment or pressure. Calm, informed support often makes treatment easier to begin.
People in Euless, Dallas, and across DFW who are looking for outpatient addiction and mental health care can learn more about options through Maverick Behavioral Health. For confidential help with MAT, Suboxone treatment, or a broader outpatient plan, call (888) 385-2051.