


The moment usually doesn’t look dramatic. It often happens in a parked car after work, in a bathroom before bed, or early in the morning after another night that got out of control. A person looks at the phone, thinks about deleting a number, thinks about waiting until Monday, and knows something has to change.
That moment matters. The first step in recovery is often described as admitting the problem, and for many people that admission is quiet, private, and painful. It can also be the start of something solid. If help is needed in Euless, Dallas, or elsewhere in the Dallas-Fort Worth area, the next few hours matter more than getting every decision perfect.
Table of Contents
- Acknowledging This Moment and What Comes Next
- Making Your First Call for Support
- The Intake Process What to Expect at Your First Assessment
- Choosing Your Path Understanding Outpatient Options in DFW
- Navigating Insurance and Family Support
- Your Recovery Starts Today in Dallas-Fort Worth
Acknowledging This Moment and What Comes Next
A person may be reading this after a spouse said they were done covering for it. Another may have missed work, scared a child, run out of excuses, or felt exhausted by trying to manage everything alone. The details vary, but the emotional mix is often the same. Fear. Relief. Shame. Hope. Uncertainty.
Choosing help isn’t proof that someone is weak. It’s proof that denial has started to loosen its grip. That matters, because people usually don’t move from full denial to full acceptance in one clean leap. Many begin recovery by slowly noticing how substance use has affected sleep, work, money, mood, parenting, or the ability to feel like themselves.

Why this decision is bigger than it feels right now
The first step in recovery has deep roots in 12-step language. Step 1 of AA says, “We admitted we were powerless over alcohol, that our lives had become unmanageable.” For some people, that wording fits immediately. For others, it takes time. Either way, honesty about what’s happening is often the point where recovery becomes possible.
There is real reason for hope. A landmark 2024 report estimated that 29.3 million U.S. adults, or 11.1% of the adult population, have resolved a significant substance use problem and are living in recovery, as summarized in this recovery overview. That means this path is not rare, strange, or out of reach.
Recovery is built by ordinary people who finally stopped trying to out-negotiate a problem that was already costing too much.
What needs to happen after the decision
The biggest mistake after deciding to get help is waiting for the “right time.” Waiting usually means more use, more secrecy, and more risk. Action lowers chaos. Even a simple phone call starts replacing panic with a plan.
Helpful immediate actions include:
- Move toward contact: Call a treatment provider, trusted family member, doctor, sponsor, or sober support today.
- Reduce access if possible: If alcohol, pills, or drug paraphernalia are nearby, get space from them and avoid being alone with them.
- Cancel nonessential obligations: A meeting, social event, or errand can wait if it interferes with getting assessed safely.
- Learn the early road ahead: Reading about the stages of recovery can help make the next phase feel less confusing.
The goal right now isn’t to solve everything. It’s to protect the next decision. Then the one after that.
Making Your First Call for Support
The first call is usually harder than the first appointment. Many people can imagine sitting in an office more easily than saying the words out loud. That’s normal. A short, honest call is enough.
A person doesn’t need a polished explanation. They don’t need to know whether they need detox, outpatient care, therapy, or medication. They only need to say enough for someone qualified to begin sorting out what comes next.
What to say when words feel stuck
Any of these opening lines work:
- Simple and direct: “I think I need help with my drinking, and I don’t know where to start.”
- If drugs are involved: “I’m using pills and I’m worried about stopping on my own.”
- If things are unclear: “Something’s wrong. I keep trying to stop and I can’t keep this under control.”
- If calling for a loved one: “Someone close to me needs help, and I need to know what to do next.”
That is enough to begin.
Practical rule: A good first call should feel like a conversation, not an interrogation.
What the person on the phone will usually ask
The questions are practical. They help determine urgency and the safest next step. A caller should expect questions such as:
- What substance is being used? Alcohol, opioids, stimulants, prescription medication, or more than one.
- When was the last use? This helps identify withdrawal risk and timing.
- Is there any immediate danger? Thoughts of self-harm, overdose risk, severe withdrawal, confusion, or inability to stay safe alone.
- What does daily life look like right now? Work, school, parenting, transportation, and housing often shape the level of care.
- Has treatment happened before? Prior attempts matter because they show what helped and what didn’t.
A caller can say “I don’t know” to any of these. Uncertainty is common at this stage.
When the call should become emergency action
Some situations are not wait-and-see situations. If someone is at risk of overdose, having severe withdrawal symptoms, experiencing seizures, hallucinations, chest pain, extreme confusion, or active suicidal thinking, immediate emergency help is the right move. In those moments, the first step in recovery is safety, not paperwork.
For non-emergency support in the Dallas-Fort Worth area, including Euless and Dallas, the next right move is to call (888) 385-2051 and ask for guidance about assessment, level of care, and what to do before arrival.
Why immediate support matters
Recovery usually gets stronger when support begins early. A 2006 Journal of Substance Abuse Treatment study found that attending at least 27 weeks of AA meetings in the first year was linked with significantly lower relapse rates, as discussed in this review of 12-step success and engagement. The practical takeaway is simple. Momentum matters. Once a person decides to get help, fast connection is better than isolated willpower.
A first call can also ask very concrete questions:
- Scheduling: “How soon can I be assessed?”
- Logistics: “Can I keep working while getting treatment?”
- Medication questions: “Do you treat opioid dependence with medication?”
- Privacy: “Who will be told that I called?”
- Insurance: “Can someone check my benefits before I commit?”
If the person calling feels embarrassed, that doesn’t mean they’re not ready. It usually means the problem has become real enough to speak aloud.
The Intake Process What to Expect at Your First Assessment
Walking into an assessment can feel exposing. Many people expect judgment. They expect a lecture. They expect to be cornered into saying things they’re not ready to say.
A good intake doesn’t work that way. It’s a structured conversation built to answer two questions. What is happening right now, and what level of care is most likely to help safely?

What gets discussed in the assessment
The appointment usually covers more than substance use alone. Each part has a purpose.
- Use history: What substances are involved, how often they’re used, how long this has been going on, and what happens when the person tries to stop.
- Mental health symptoms: Depression, anxiety, panic, trauma symptoms, mood swings, sleep disruption, and concentration problems affect treatment planning.
- Medical and safety concerns: Current medications, withdrawal concerns, pregnancy status if relevant, and immediate safety issues.
- Daily functioning: Work performance, school, parenting demands, housing, transportation, and legal or relationship stress.
- Treatment goals: Some people want abstinence immediately. Others arrive unsure. That honesty helps create a realistic starting point.
Why dual diagnosis screening matters early
A lot of people hesitate during intake because substance use doesn’t feel like the whole story. Depression may feel like the underlying issue. Trauma may feel older and heavier. Anxiety may have been there long before the drinking or drug use escalated.
That’s why integrated screening matters. For dual diagnosis populations, individuals may resist acknowledging substance use as “the problem” when untreated depression or trauma feels like the primary driver, making integrated screening during intake essential to address the root causes of addiction, as explained in this discussion of Step One and co-occurring mental health challenges.
Sometimes the most important sentence in intake is, “Both things can be true.”
A person can be struggling with addiction and still need serious attention for trauma, panic, grief, or depression. Treating only one side usually leaves the other side waiting to pull them backward.
How to prepare before walking in
The assessment tends to go more smoothly when a person brings a few basics:
- Identification and insurance card: If available, bring both.
- Medication list: Include prescribed medications and recent changes.
- A rough use timeline: It doesn’t need to be exact. Approximate patterns help.
- Emergency contact information: If the person wants a family member or support person involved.
- Questions written down: Anxiety makes people forget what they meant to ask.
Some people also benefit from reviewing practical expectations before they arrive. A short guide on how to prepare for your first therapy session can make the process feel less unfamiliar.
Financial questions may also come up during intake, but they usually don’t have to be solved on the spot. The assessment is first about safety, clarity, and fit. Once those are clear, the rest becomes easier to handle.
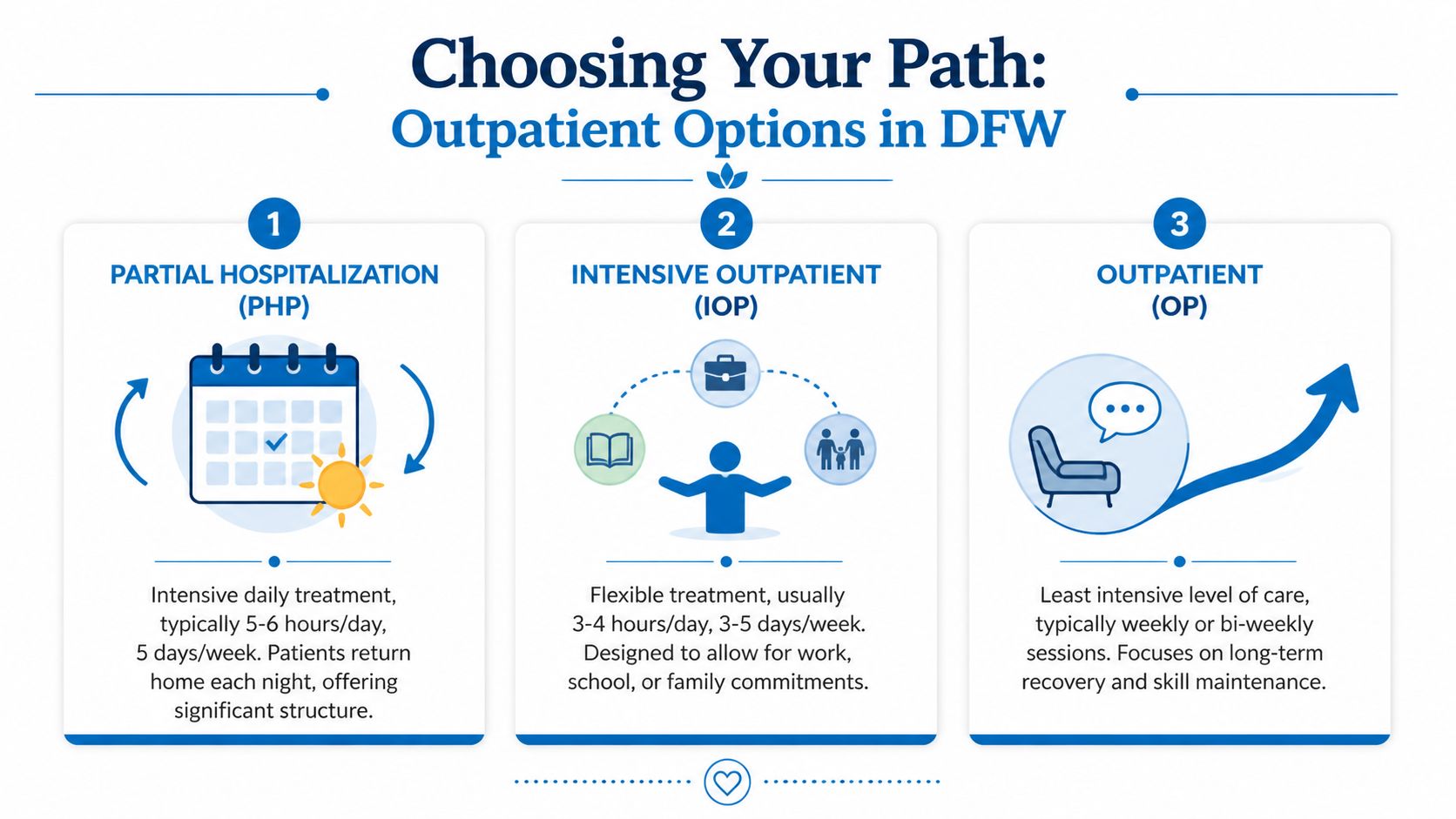
Choosing Your Path Understanding Outpatient Options in DFW
Not everyone needs the same intensity of treatment. Some people need a highly structured schedule after a crisis. Others need solid treatment that fits around work, school, or parenting. That’s one reason outpatient care matters in Dallas-Fort Worth. It gives people more than one way to begin.
The right level of care depends on stability, withdrawal risk, home environment, mental health needs, relapse history, and how much outside support is available. What works for one person may be too little or too much for another.
Comparing outpatient levels of care
| Comparing Outpatient Treatment Levels at Maverick Behavioral Health | |||
|---|---|---|---|
| Level of Care | Time Commitment | Best For Individuals Who… | Core Focus |
| Partial Hospitalization | Most of the day, several days each week | Need strong structure and frequent clinical support, but don’t need overnight care | Stabilization, routine, therapy, relapse prevention, close monitoring |
| Intensive Outpatient | Several hours per day on multiple days each week | Need meaningful treatment while still managing work, school, or family responsibilities | Skill building, group therapy, accountability, relapse prevention in real life |
| Outpatient | Usually fewer sessions each week | Are more stable and need ongoing support, step-down care, or long-term maintenance | Continued therapy, recovery maintenance, coping skills, aftercare support |
How to think about the trade-offs
PHP gives more structure. That can help when cravings, mood instability, or home stress are still intense. The trade-off is time. It asks more from the schedule.
IOP is often the middle ground. It allows a person to practice recovery while still living daily life. The trade-off is that freedom can expose weak spots quickly. If the home environment is chaotic, IOP may not be enough by itself.
Standard outpatient works best when the person already has some stability and can use therapy consistently without needing intensive oversight. The trade-off is obvious. If symptoms are severe, weekly support may be too thin.
Where medication-assisted treatment fits
For opioid use, medication-assisted treatment can make the first step in recovery more realistic. It can reduce the chaos of cravings and withdrawal so the person is able to participate in counseling, groups, and daily responsibilities. In practical terms, medication doesn’t replace recovery work. It often makes recovery work possible.
Recovery pathway data reflects that role. For alcohol, 1.6 million people are in early recovery, defined as less than 1 year, and 2.6 million are in mid-recovery, defined as 1 to 5 years. For opioids, 26% of early recoverers use MAT, rising to 42% in mid-recovery, as noted in this summary of recovery indicators and pathways.
That doesn’t mean medication is right for every case. It does mean people with opioid dependence shouldn’t assume they must white-knuckle their way through treatment to be doing recovery “correctly.”
The best treatment plan is the one a person can engage in honestly, safely, and long enough for change to take hold.
In the Dallas-Fort Worth area, some outpatient programs include PHP, IOP, standard outpatient care, dual diagnosis support, and MAT with Suboxone. Maverick Behavioral Health is one example of a provider offering those outpatient options for adults in Euless, Dallas, and surrounding communities.
Navigating Insurance and Family Support
Two worries stop a lot of people after they’ve already decided to get help. The first is money. The second is family.
Both can feel heavy enough to delay treatment. Neither should be allowed to make the decision by default.
How to handle insurance without getting overwhelmed
Insurance verification is usually much simpler than people expect. The first step is gathering the card and making the call. Admissions staff can usually explain what information is needed and what the next financial conversation will look like.
A straightforward approach looks like this:
- Start with the basics: Have the insurance card, legal name, date of birth, and contact number ready.
- Ask for a benefits check: Don’t guess what’s covered. Ask for verification.
- Clarify level of care questions: Coverage can differ for assessment, therapy, medication visits, and different outpatient levels.
- Ask what happens next: If there are out-of-pocket responsibilities, request a clear explanation before scheduling.
A person who wants a clearer picture before calling can review how to find out if insurance will pay for treatment. That often makes the financial conversation feel less intimidating.
How to involve family without losing control of the process
Some family members are supportive right away. Others are angry, skeptical, frightened, or exhausted. All of that can exist at once. A person starting treatment doesn’t need to solve every relationship issue before entering care.
It helps to decide what kind of involvement is useful.
- One trusted contact: Sometimes one calm, reliable person is more helpful than a large family discussion.
- Practical support first: Transportation, childcare help, schedule coverage, or accountability may matter more than emotional speeches.
- Boundaries matter: A loved one can be informed without being put in charge.
- Family therapy can help later: Structured conversations tend to work better than emotional confrontations at home.
Support helps when it lowers chaos. It hurts when it turns into monitoring, arguing, or punishment.
Confidentiality matters here. Treatment is private, and the person in care should understand who can be involved, what can be shared, and what remains confidential. That control often reduces the fear that asking for help means losing autonomy.
If a family member wants details the person isn’t ready to share, that’s not proof treatment isn’t working. Early recovery often needs privacy, consistency, and space to stabilize before damaged relationships can be repaired well.
Your Recovery Starts Today in Dallas-Fort Worth
A person doesn’t need to feel fully ready to take the first step in recovery. They only need to be willing to interrupt the pattern that’s been running their life. Readiness often grows after action, not before it.
The practical next move is simple. Call. Ask what level of care makes sense. Be honest about recent use, safety concerns, work obligations, and mental health symptoms. If the situation feels urgent, say so immediately. If the person feels ashamed, say that too. It won’t shock anyone.
People in Euless, Dallas, and across the Dallas-Fort Worth metroplex often need treatment that fits real life. That may mean outpatient care instead of overnight treatment. It may mean an assessment first, then a decision about PHP, IOP, outpatient therapy, or medication support. It may also mean beginning with crisis planning if withdrawal or overdose risk is part of the picture.
The key is not to stall at the exact point where courage finally showed up.
Call Maverick Behavioral Health at (888) 385-2051 if help is needed now. That phone call can clarify safety, scheduling, insurance questions, and what to bring to the first assessment. For many people, the hardest part is the minute before dialing. After that, the process becomes concrete.
Recovery doesn’t start when everything is fixed. It starts when a person stops trying to manage it alone and takes the next clear step.
If help is needed for drug or alcohol addiction in Euless, Dallas, or the surrounding metroplex, Maverick Behavioral Health can help with confidential guidance on assessment, outpatient treatment options, insurance verification, and next steps. Call (888) 385-2051 to speak with someone about getting started today.