


A person in Dallas-Fort Worth often starts the search late at night. A spouse is worried. A parent is exhausted. A working professional is trying to keep life together while alcohol, pills, or another drug keeps making things worse. They search for archway recovery services because they've heard that strong programs offer more than a quick fix.
That search usually means something important. It means they aren't looking for just any rehab. They're looking for a program that feels organized, evidence-based, and capable of treating the whole person.
For people in Euless, Dallas, and the surrounding DFW area, a key question isn't whether a California program sounds good. The core question is what makes a program like that work, and where that same level of care can be found close to home. The right local option should make treatment easier to start, easier to fit into real life, and easier to continue after the first phase of recovery.
Table of Contents
- Finding Hope and Healing in Dallas-Fort Worth
- What to Look For in a Premier Treatment Center
- From PHP to IOP A Guide to Outpatient Care Levels
- Why Dual Diagnosis and MAT Are Critical for Success
- Making Treatment Affordable Your Financial Options
- What to Expect from the Admissions Process
- Your Questions About Treatment Answered
Finding Hope and Healing in Dallas-Fort Worth
Searching for archway recovery services usually reflects a deeper need. The person searching wants proof that a treatment center can do more than offer a few counseling sessions. They want structure, trained clinicians, and a clear path forward.
In DFW, that matters because life doesn't pause for recovery. Many adults still need to manage work, parenting, school, court requirements, or family responsibilities while getting help. A good program has to meet that reality instead of ignoring it.
Why local care matters
A local program gives people a better chance to stay engaged. They can attend treatment while remaining connected to their support system, their home environment, and the practical parts of life that still need attention. That often makes the next step feel less overwhelming.
It also makes assessment more useful. When a treatment team understands the pressure points a person is facing, such as commuting across Dallas, managing childcare in Euless, or trying to return to work, they can recommend a level of care that fits the person instead of forcing the person to fit the program.
A program only helps if a person can start it, stick with it, and keep building on it after the first crisis passes.
Many readers get stuck on one question. They wonder whether they need residential treatment, outpatient treatment, or something in between. That confusion is normal. Many individuals aren't experts in addiction treatment language, and they shouldn't have to be before asking for help.
What this search should lead to
The best use of an archway recovery services search isn't a long comparison between facilities in different states. It's using that search to identify what quality looks like. That includes thoughtful assessment, evidence-based therapy, support for co-occurring mental health needs, and a plan for what happens after early recovery.
That standard can absolutely be found in the Dallas-Fort Worth area.
For someone who feels scared, ashamed, or worn down, the next step doesn't need to be dramatic. It only needs to be clear. Learn what quality care looks like, identify the right level of support, and then reach out for a confidential conversation about treatment options nearby.
What to Look For in a Premier Treatment Center

Some treatment centers sound impressive until a family asks simple questions. What level of care is available? What happens after discharge? How are mental health needs handled? If the answers are vague, that's a warning sign.
Programs modeled after established community-based recovery organizations tend to build trust through consistency and breadth of care. In one example, a nonprofit recovery provider reported estimated annual revenue of $256,665 and received a state grant award exceeding $213,000 to expand Enhanced Care Management for high-need clients in Solano County, showing both operational scale and community investment through documented nonprofit and grant reporting.
A strong program treats recovery as a process
Addiction treatment shouldn't stop at intake or detox. A premier center should think in stages.
That means a person is assessed carefully, placed into the least intrusive level of care that still matches clinical needs, and moved up or down as progress changes. Some people need daily structure at first. Others need several therapy sessions each week while living at home. Others are stepping down from a higher level of care and need support to stabilize.
A strong center often includes:
- Thoughtful assessment: The program should determine what level of care fits the person, not just fill the next open slot.
- More than one service type: Counseling alone may not be enough. Many people also need family support, life-skills work, trauma-informed care, or help reconnecting with work and housing.
- A long-view mindset: Recovery isn't just stopping use. It's rebuilding stability, emotional regulation, and daily functioning.
Clinical quality should be visible
Clinical quality shouldn't be hidden behind marketing language. Families should be able to identify actual treatment approaches and understand how care is delivered.
For example, archway recovery services is described as offering cognitive behavioral interventions, motivational approaches, trauma-informed care, psychoeducation, and support for personal, social, and cultural needs through a broad continuum of care in published program information. That kind of detail matters because it shows how treatment is carried out, not just what buzzwords are used.
A center should also be accountable. In the same public profile, that provider is listed with a Recovered TrustScore of 3.5/5 and support for adults and young adults with specialized tracks for certain populations. Publicly visible ratings and service descriptions don't tell the whole story, but they help families see whether a program operates with some transparency.
Practical rule: If a program can't explain how it assesses people, what therapies it uses, and what support looks like after treatment, it may not be ready to guide long-term recovery.
The best treatment centers don't promise perfection. They offer clarity. They show how people enter care, how treatment is customized, and how support continues when the early momentum of rehab starts to wear off.
From PHP to IOP A Guide to Outpatient Care Levels
Outpatient treatment often confuses families because the terms sound technical. PHP, IOP, outpatient. To someone in crisis, they can all blur together.
The easiest way to understand them is to think of recovery support like a set of training wheels that gradually change. At first, a person may need more structure and more contact. As stability improves, the support can loosen without disappearing.
How the step-down model works
A flexible continuum is one of the strongest signs of modern treatment. Archway's published model describes care that can move from more intensive treatment to outpatient and alumni support, and its residential programming is described as ranging from 14 to 90 days, typically 30 days, in its continuum overview. That step-down structure matters because it helps reduce abrupt disruptions between levels of care.
For DFW residents seeking a local equivalent, the same idea applies in outpatient settings.
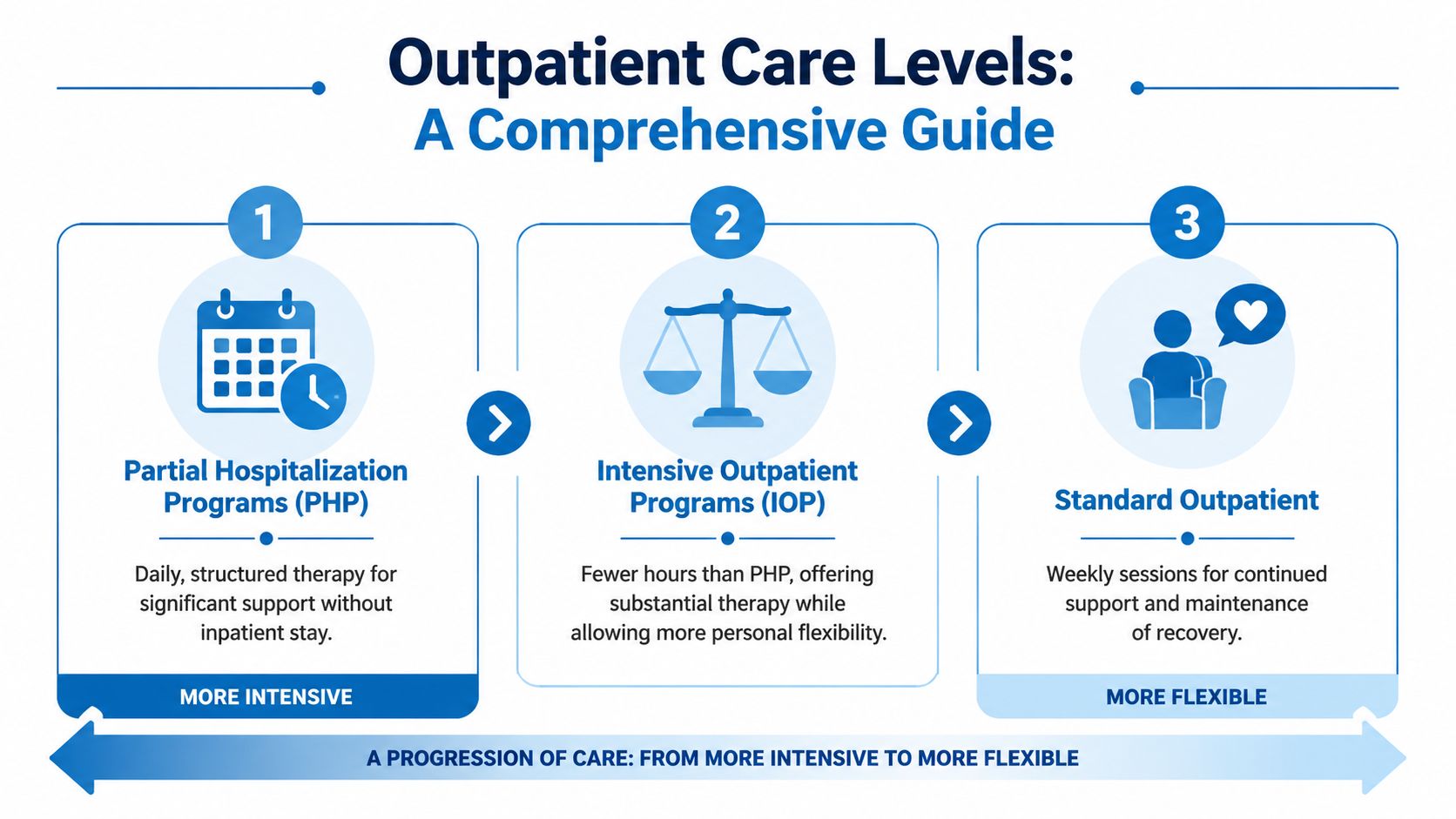
PHP usually fits people who need a high level of support but don't require an inpatient stay. They attend structured treatment for much of the day and return home afterward. This level can help when cravings are strong, daily functioning has become unstable, or a person is stepping down from residential care.
IOP offers substantial clinical support with more flexibility. It works well for adults who need regular therapy and accountability but also need to maintain work, school, or family responsibilities. Readers who want a deeper breakdown can review this guide on what IOP therapy means in practice.
Standard outpatient is usually the least intensive level. A person may attend weekly sessions, continue individual therapy, and focus on maintaining gains already made in higher levels of care.
The right question isn't “Which program sounds best?” It's “Which program matches what this person needs right now?”
PHP vs IOP Choosing Your Level of Support
| Feature | Partial Hospitalization (PHP) | Intensive Outpatient (IOP) |
|---|---|---|
| Overall structure | More intensive and more frequent treatment | Strong support with greater schedule flexibility |
| Best fit | People needing daily stability and close monitoring | People who are stable enough to live at home and manage more independence |
| Daily life impact | Treatment takes up a larger part of the week | Easier to balance with work, school, or parenting |
| Therapy focus | Intensive group and individual work, skill-building, relapse prevention | Continued therapy, coping skills, accountability, and transition planning |
| Common use | Early treatment or step-down from residential care | Step-down from PHP or direct entry for moderate support needs |
Many people choose the wrong level because they focus on convenience first. That's understandable, but risky. A person who needs more support may struggle in a program that's too light. A person who is stable may feel discouraged by more intensity than necessary.
A quality assessment helps sort that out quickly. The goal isn't to put everyone into the same box. The goal is to match care to the person's current condition and then adjust as recovery strengthens.
Why Dual Diagnosis and MAT Are Critical for Success

A person may say drinking is the problem. Another may say opioids are the problem. A family may focus on cocaine, meth, or prescription pills. Sometimes that's true, but it's often only part of the picture.
Many adults use substances alongside anxiety, depression, trauma, panic, grief, or other mental health symptoms. When treatment ignores that connection, recovery becomes harder to hold onto.
Why mental health and substance use must be treated together
This is what clinicians mean by dual diagnosis. It doesn't mean a person is unusually complicated. It means treatment has to reflect reality.
Archway's clinical model describes an integrated approach that uses the American Society of Addiction Medicine Criteria and assesses six domains during care planning, including withdrawal risk, biomedical conditions, emotional and behavioral conditions, readiness for change, relapse risk, and recovery environment in its clinical overview. That kind of assessment matters because substance use rarely exists in isolation.
When care is integrated, the treatment team doesn't force a person to fix one problem and then come back later for the other. Therapy can address cravings, shame, sleep disruption, trauma triggers, depression, family conflict, and relapse prevention as connected issues.
That matters in everyday terms. A person with untreated panic may keep drinking to calm down. A person with trauma symptoms may keep using opioids to avoid emotional pain. If the emotional driver remains untouched, substance use often returns.
What MAT actually means
Medication-Assisted Treatment, or MAT, is another area where families often feel uncertain. Some still worry that medication means a person isn't really in recovery. That misunderstanding keeps people from effective care.
MAT uses approved medications to reduce withdrawal symptoms, lower cravings, and give the brain and body enough stability for therapy to work. It's especially important in opioid and alcohol treatment. It doesn't replace counseling. It supports counseling.
For readers who want a plain-language breakdown, this resource explains what medication-assisted treatment involves.
A helpful way to think about MAT is this: if a person is constantly battling withdrawal, intense cravings, or fear of getting sick, they may not be emotionally available for therapy. Medication can create enough steadiness for real clinical work to begin.
- Dual diagnosis care helps identify what fuels use beneath the surface.
- MAT support can reduce the physical chaos that makes early recovery fragile.
- Integrated planning gives both pieces attention at the same time.
Treatment is stronger when it answers two questions together. What is the person using, and what pain or instability keeps driving that use?
When a local DFW program offers both dual diagnosis treatment and MAT, it's not adding extras. It's meeting the standard that many people need for recovery to last.
Making Treatment Affordable Your Financial Options
Cost stops many people before treatment even starts. Some delay the call because they assume rehab will be out of reach. Others fear getting pressured into a commitment before they understand coverage.
A better approach starts with information. Public descriptions of programs like archway recovery services show how cost transparency can remain limited, which creates barriers for people already under stress. In Texas, where many adults are uninsured, a confidential benefits check is often the most practical first step, as noted in this discussion of payment barriers and admissions questions.
The first call should answer financial questions
Families don't need to arrive with every insurance detail figured out. An admissions team should help sort through the basics. That usually includes whether a plan is active, what level of care may be covered, and what next steps make sense.
Can treatment be affordable?” is often the wrong first question. The more useful question is “What does this specific policy allow, and what options are available right now?
Readers who want a broader look at common payment paths can review how to pay for drug rehab.
What families should ask
A short list of financial questions can make the process less intimidating:
- Insurance compatibility: Is the plan likely to work with the recommended level of care?
- Out-of-pocket expectations: Are there deductibles, copays, or other expenses to prepare for?
- Level-of-care impact: Does coverage differ between PHP, IOP, and standard outpatient?
- Admissions timing: How long might authorization or verification take?
A quality admissions conversation should feel calm and factual. It shouldn't feel rushed or evasive.
For many people in DFW, financial clarity is what turns a vague idea into a real start date. Once the unknowns are reduced, treatment often feels much more possible.
What to Expect from the Admissions Process
The admissions process feels less scary when a person knows what happens next. Most hesitation comes from uncertainty, not unwillingness. A clear process lowers that pressure.

Step one the first phone call
When someone calls (888) 385-2051, the first conversation should be confidential, calm, and focused on understanding the situation. The admissions professional may ask what substances are involved, whether mental health symptoms are present, whether there has been recent treatment, and what kind of support the caller needs right now.
That call isn't a test. A person doesn't need perfect words or a polished explanation. “Things are getting worse,” “there's been a relapse,” or “work is falling apart” is enough to begin.
Important: The first conversation should feel like guidance, not a sales script.
Some callers are family members. That's common. A spouse, parent, sibling, or adult child may be the one gathering information first. They can still get a clear picture of what treatment may look like.
Step two and step three verification and assessment
After the initial call, the next step is usually insurance verification or a discussion of payment options. That helps the admissions team explain what levels of care may be realistic and how quickly a person can begin.
Then comes the clinical assessment. This part matters because symptoms, risk level, mental health history, substance use pattern, home environment, and past treatment all affect placement. A careful assessment helps determine whether a person belongs in PHP, IOP, or standard outpatient care.
A simple version of the process looks like this:
- Confidential call: Share what's happening and ask immediate questions.
- Benefits review: Check insurance or discuss private-pay options.
- Clinical assessment: Match the person to the right level of care.
By the time those steps are complete, the path usually feels more manageable. Instead of facing a fog of uncertainty, the person has names for the options, a recommendation, and a plan to start.
Your Questions About Treatment Answered
Even after someone understands levels of care, a few practical fears often remain. These questions are common, and they deserve direct answers.
Can a person keep treatment private
In most cases, yes. Confidentiality is a core part of behavioral health care. Working professionals often worry that treatment will automatically become visible to employers, coworkers, or clients. That fear keeps many people from reaching out.
The safest move is to ask specific privacy questions during admissions. A quality program should explain confidentiality rules clearly, discuss communication preferences, and help the person understand how scheduling and documentation work.
Can treatment work around a job or school
Often, yes. This is one reason outpatient care matters so much in the Dallas-Fort Worth area. PHP and IOP are designed to offer structure without requiring a person to disappear from everyday life entirely.
That said, flexibility shouldn't come at the cost of getting enough support. If someone is trying to protect work at all costs, they may choose a level of care that's too light. It's better to be honest during assessment and let the clinical team recommend the right fit.
Does family involvement matter
For many people, it does. Family can provide accountability, transportation, emotional support, and a more stable home environment. Family work can also help repair communication patterns that became strained during active substance use.
Not every family situation is healthy or available, and treatment should respect that. But when family involvement is appropriate, it often strengthens recovery.
What happens after the program ends
This question is one of the most important. Some programs mention alumni support without defining it. That's not enough.
A stronger standard is a structured aftercare plan with ongoing support, relapse prevention strategies, and a practical reintegration plan; relapse rates can be 40 to 60 percent within the first year without adequate aftercare, as noted in this discussion of aftercare and long-term recovery planning.
A useful aftercare plan may include:
- Continued therapy: Ongoing individual or group support after the main program ends.
- Relapse prevention planning: Specific strategies for triggers, cravings, and high-risk situations.
- Community reintegration: Support for work, relationships, accountability, and daily routine.
- Recovery connection: Alumni groups, check-ins, or other ways to stay engaged.
The key point is simple. Treatment shouldn't end with discharge. It should continue in a form that helps the person protect what they've built.
For people in Euless, Dallas, and the wider DFW area who are looking for the same kind of complete care they hoped to find through an archway recovery services search, Maverick Behavioral Health offers outpatient treatment built around real life. The team provides individualized support across PHP, IOP, standard outpatient care, dual diagnosis treatment, and MAT, with a compassionate admissions process that starts with a confidential call. To speak with someone about treatment options, insurance, or the right next step, call (888) 385-2051.