


A lot of people reach this point in the same way. They haven't planned a perfect quit date. They're exhausted, scared by what meth is doing to their sleep, their mood, their work, or their family, and they know something has to change now.
Family members often feel just as overwhelmed. They may be asking whether this is something that can be handled at home, whether a loved one needs detox, whether the person is dealing with addiction alone or with depression, anxiety, or psychosis too. Those questions are common, and they matter because detox from methamphetamine is less about “getting it out of the system” and more about getting through a risky crash safely.
Table of Contents
- The Moment You Decide It's Time for a Change
- The Methamphetamine Withdrawal Timeline and Symptoms
- Why Toughing It Out Is Not a Safe Option
- Choosing Between Inpatient and Outpatient Detox
- A Closer Look at Outpatient Detox in DFW
- How to Get Meth Detox Help in Dallas and Euless
- Your Next Step Is the Most Important One
The Moment You Decide It's Time for a Change
For many adults, the decision doesn't feel brave at first. It feels messy. Someone looks in the mirror after days of barely sleeping, or a parent notices how fast paranoia and isolation have taken over, or a partner realizes the same promises keep ending the same way. They know meth can't stay in the picture, but they don't know what stopping will look like.
That uncertainty keeps people stuck. Some fear the crash. Others fear what happens if they ask for help and get judged. Some tell themselves they should be able to manage it alone, even while noticing clear signs of meth addiction in daily life, relationships, and mental health.
A practical starting point is recognizing that substance use concerns and mental health concerns often show up together. For people wondering whether mood changes, anxiety, isolation, or loss of control mean it's time for support, this guide on recognizing therapy signals offers a useful outside perspective on when professional help makes sense.
Getting help for meth use isn't a sign that someone has failed. It's a sign that the problem has become too serious to keep handling with guesswork.
In Dallas, Euless, and across DFW, the safest next move is usually not to debate the problem for another week. It's to get a real assessment. Once someone understands whether they need detox, psychiatric support, outpatient treatment, or a higher level of care, the situation becomes more manageable. Fear drops when the plan gets clearer.
The Methamphetamine Withdrawal Timeline and Symptoms
A lot of people expect meth withdrawal to be a short, miserable weekend. In real life, the timeline is less tidy. The first crash can be intense, but the period after the crash is often where families misread the risk and assume the person is out of danger.
What usually happens first
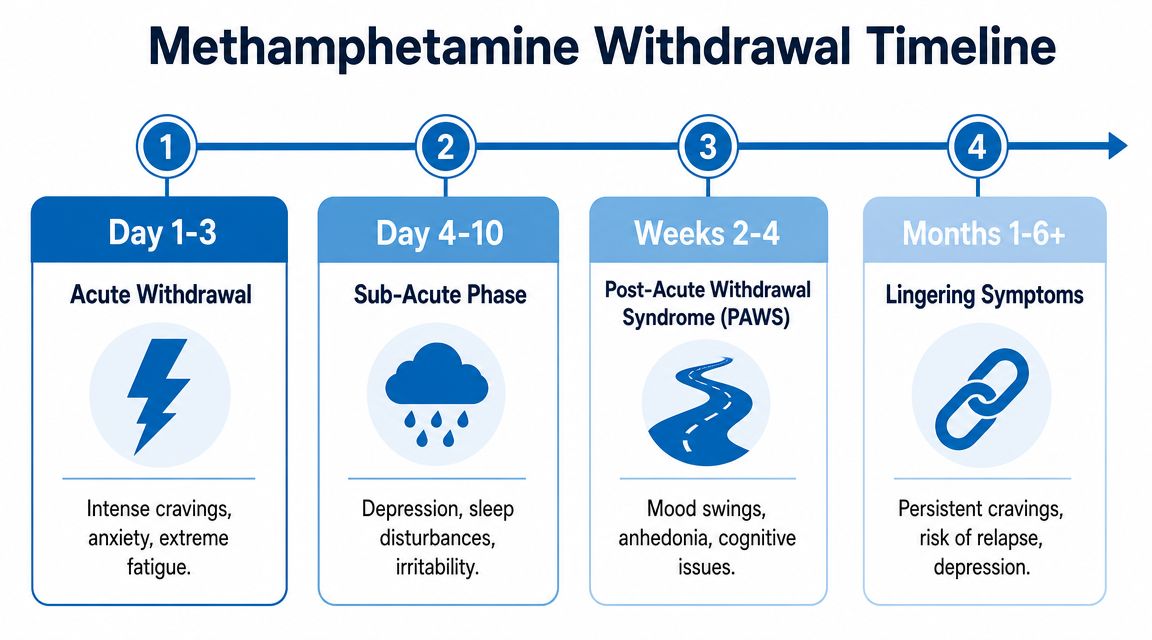
Methamphetamine withdrawal often starts within the first day after the last use. Early symptoms commonly include extreme fatigue, long periods of sleep, increased appetite, irritability, low mood, anxiety, and strong cravings. Some people look physically calmer within a day or two, but that can be misleading because emotional distress and poor judgment may still be building.
In practice, the first stage often feels like a hard neurological drop. The body is no longer being pushed by a stimulant, so energy crashes. The brain can swing in the opposite direction, leaving the person flat, agitated, hopeless, or unable to feel much of anything.
There is no FDA-approved medication designed specifically for methamphetamine detox. Care is usually supportive and based on what the person in front of you is dealing with, such as insomnia, dehydration, agitation, paranoia, or psychosis. That is one reason a proper assessment matters so much, especially if someone in DFW is trying to decide whether outpatient support is enough or whether they need a higher level of care first.
What tends to happen over the next two weeks
Clinical research on abstinent methamphetamine-dependent adults found that withdrawal symptoms often peak early, then decline through an acute and subacute phase, with many depressive symptoms, appetite changes, and craving-related symptoms settling substantially within about the first two weeks of abstinence, according to this NCBI study on methamphetamine withdrawal patterns.
That pattern is helpful, but it should not be oversimplified. Improvement is common. Stability is not guaranteed.
A practical way to look at the first two weeks:
- First 24 hours: The crash begins. Sleepiness, exhaustion, hunger, and low mood are common.
- Days 2 to 3: Symptoms often feel heaviest here. Depression, agitation, and cravings can hit hard.
- Days 4 to 7: The body may start settling, but sleep, motivation, and concentration are often still off.
- Week 2: Many acute symptoms begin to ease, yet cravings, emotional numbness, and poor follow-through can still interfere with recovery.
This is the stage where treatment planning becomes practical, not theoretical. Someone may no longer need round-the-clock observation, but they may still need daily structure, medication review, psychiatric support, urine drug screening, and several hours of treatment each week to avoid an immediate return to use. For adults in the Dallas-Fort Worth area, that is often the point where the choice between inpatient care and a well-built outpatient program becomes clearer.
What families often misunderstand
One peer-reviewed study of recently abstinent methamphetamine users found that depression, anxiety, and withdrawal symptoms dropped significantly over the first two weeks of residential abstinence, with the biggest improvement during the first week. The same study also found that cravings often lasted well beyond the initial crash, as reported in this peer-reviewed study on withdrawal and cravings.
That matches what clinicians see. A person may be sleeping more, eating again, and talking more normally by the end of the first week. Family members take a breath and assume the crisis has passed. Then the person goes home, gets bored, feels ashamed, runs into stress, or starts thinking they can control it this time.
Practical rule: Looking better after a few days does not mean the relapse risk is low.
Meth withdrawal is usually less about a dramatic physical emergency and more about how quickly depression, cravings, impulsivity, and mental health symptoms can pull someone back into use. That is why the timeline matters. It helps determine who may be appropriate for outpatient detox with strong support, and who needs inpatient care before stepping down.
Why Toughing It Out Is Not a Safe Option
A lot of people assume meth withdrawal is mainly a comfort issue. They expect exhaustion, appetite changes, and low mood, and they tell themselves they can endure it on the couch. That thinking misses the part that often creates the most danger.

The risk is often psychiatric, not dramatic physical collapse
The most dangerous part of meth detox is often not a classic medical reaction but the risk of severe psychiatric symptoms. For people with co-occurring conditions, withdrawal can trigger or worsen depression and suicidality, making professional dual-diagnosis assessment and support a critical safety measure, as reflected in SAMHSA's mental health and substance use support guidance.
That matters because meth can blur the picture. A person may already have depression, anxiety, trauma symptoms, paranoia, or psychosis. Meth may intensify those symptoms, temporarily mask them, or make them harder to assess. Once use stops, the person may look “cleaner” physically while becoming more unstable emotionally.
This is why home detox often goes wrong. Family members watch for sweating, shaking, or vomiting because those are the signs they associate with withdrawal. Meanwhile, a more serious danger may be hopelessness, panic, suspicious thinking, severe agitation, hearing or seeing things, or talking like life isn't worth continuing.
Red flags that need urgent attention
These signs call for immediate professional evaluation:
- Suicidal thinking: Talking about wanting to die, not wanting to wake up, or feeling like everyone would be better off without them.
- Psychosis: Hearing voices, seeing things, intense paranoia, or fixed false beliefs.
- Severe depression: Inability to get out of bed, complete emotional shutdown, or profound despair.
- Unsafe behavior: Wandering, aggression, impulsive actions, or inability to follow basic safety directions.
- No stable supervision: Being alone, staying in an unsafe environment, or being around people still using meth.
If a person cannot be kept safe at home, the question is no longer whether detox is uncomfortable. The question is where they can be stabilized safely.
“Toughing it out” usually sounds appealing because it looks simple and private. In reality, it often means unmanaged cravings, poor sleep, isolation, and no trained eyes on worsening mental health symptoms. For adults with any history of psychiatric instability, the safer choice is supervised care with the ability to step up treatment quickly if symptoms escalate.
Choosing Between Inpatient and Outpatient Detox
A common DFW question sounds simple: should I stay home and get help, or do I need to go somewhere and be monitored around the clock? The answer depends on risk, stability, and what will happen after today. I tell families to focus less on preference and more on whether the person can stay safe, sleep, eat, show up for care, and avoid immediate return to meth use in their current environment.
Meth detox is usually supportive care rather than a medication-driven process. That matters because adults do not all need the same setting. Some need the containment of inpatient care for a few days. Others can do well in the community if they have close clinical follow-up, a sober place to stay, and a treatment team that can respond quickly if symptoms worsen.
When inpatient usually makes more sense
Inpatient or residential detox is the safer choice when supervision cannot be left to chance.
That usually includes people with psychosis, suicidal thinking, severe agitation, extreme insomnia, or a pattern of using again within hours when meth is available. I also worry about adults who say they want help but cannot stay organized enough to attend appointments, answer calls, or follow basic safety instructions. In those cases, the structure of a controlled setting does real work. It reduces access to meth, allows staff to monitor mental status closely, and gives the person time to stabilize before bigger treatment decisions are made.
Home conditions matter just as much as symptoms. If the person will be going back to a house where others are using, where conflict is constant, or where no reliable adult can monitor them, outpatient detox may fail for reasons that have nothing to do with motivation.
When outpatient can be appropriate
Outpatient detox can be a good fit for an adult who is medically stable, not actively psychotic or suicidal, has a safe and sober place to stay, and can keep frequent appointments. It is often a practical option for people trying to protect work, parenting, or school responsibilities without stepping away from daily life completely.
The trade-off is straightforward. Outpatient care gives more flexibility, but it asks more of the patient and the home environment. Someone has to notice if sleep disappears, depression deepens, paranoia returns, or cravings start driving impulsive decisions. Families comparing levels of care often benefit from a plain-language review of the difference between inpatient and outpatient treatment.
Here is a practical way to sort the choice:
| Factor | Inpatient Detox | Outpatient Detox |
|---|---|---|
| Psychiatric status | Better for severe depression, paranoia, psychosis, or suicidal risk | Better for stable mood and thought process with close follow-up |
| Home setting | Better when home is unsafe, chaotic, or tied to drug use | Better when home is sober, calm, and dependable |
| Supervision | Staff monitor the person day and night | Monitoring happens through scheduled visits and family support |
| Access to meth | Lower immediate exposure to dealers, peers, and triggers | Higher exposure, which raises the need for accountability |
| Daily responsibilities | Work, school, and home duties usually pause | Some responsibilities can continue if the person is stable enough |
| Best fit | Higher-risk adults who need containment | Lower-risk adults who can follow through consistently |
In the Dallas-Fort Worth area, this decision should also include a practical question: if outpatient is chosen, what level of outpatient care is available right now? A weak plan with one occasional check-in is not enough for early meth withdrawal. A stronger option may involve same-week assessment, several treatment contacts per week, family communication when appropriate, and dual-diagnosis support for depression, anxiety, trauma, or stimulant-induced psychiatric symptoms. Families who want a clearer picture of what structured outpatient care can look like can review guidance from Addiction Resource Center.
A good assessment should be specific. It should ask about recent meth use, sleep over the last several days, current mood, psychosis history, other substances, transportation, home stability, and whether the person has followed through with treatment before. The safest recommendation is the one that matches the actual level of risk, even when it is less convenient.
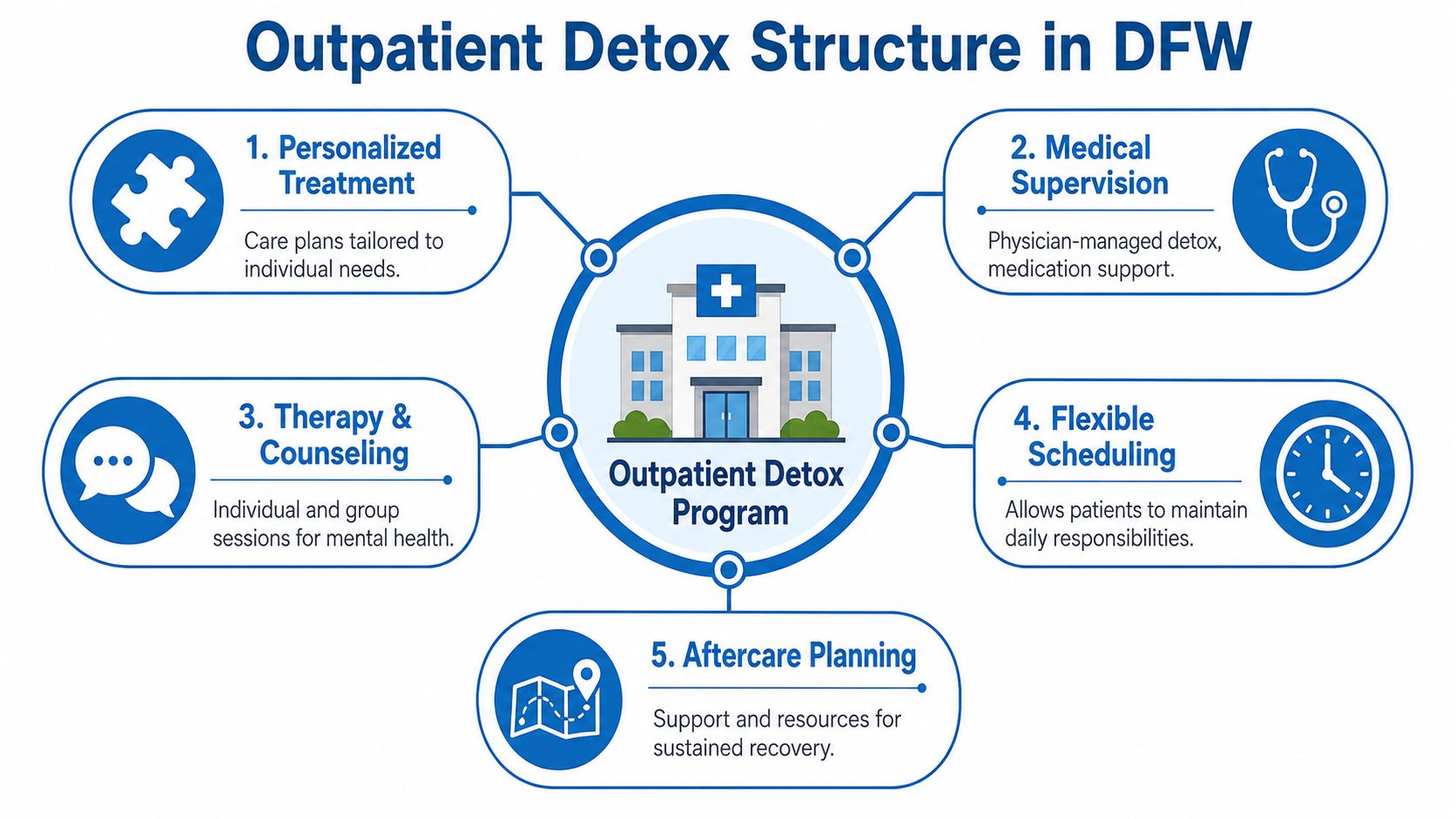
A Closer Look at Outpatient Detox in DFW
Outpatient detox in DFW works best when it's treated as a structured clinical process, not as a loose recommendation to “rest at home and check in if needed.” Strong outpatient care gives people enough support to get through the crash while staying connected to ongoing treatment after the first hard stretch.
What strong outpatient care actually includes
There isn't a medication that cures meth withdrawal. Effective methamphetamine treatment focuses on symptom management and structured support, and evidence-based outpatient programs do that through behavioral therapies and contingency management after the acute phase is addressed, as described in this NCBI overview of treatment for stimulant use disorders.
In practical terms, quality outpatient care usually includes:
- Frequent clinical contact: Early visits are close enough together to catch worsening depression, agitation, insomnia, or relapse risk.
- Dual-diagnosis evaluation: The team looks at substance use and mental health together, not as separate problems.
- Individual counseling: Sessions focus on triggers, distorted thinking, coping skills, and immediate problem-solving.
- Group treatment: Patients practice recovery skills with other adults facing similar patterns of cravings, shame, secrecy, and relapse pressure.
- Family involvement when appropriate: Loved ones learn what support helps and what accidentally makes the cycle worse.
For readers who want a broader consumer overview of what outpatient care can look like day to day, the Addiction Resource Center has a useful explanatory article.
What a week of care may involve
The level of care matters. PHP usually provides a higher degree of daytime structure and monitoring. IOP offers a step down in intensity while still keeping treatment active and frequent. Standard outpatient tends to fit later, when the person has better stability and stronger recovery footing.
A typical treatment week may combine several moving parts rather than one long therapy conversation:
- Clinical check-ins early in recovery to assess sleep, nutrition, cravings, mood, and safety.
- Skills-based therapy focused on relapse prevention, emotional regulation, and trigger management.
- Case coordination for work notes, family communication, psychiatric referral, or step-up to a higher level of care if needed.
- Aftercare planning so the patient doesn't finish the crash phase and then drift.
One local option in this category is outpatient drug rehab through programs such as PHP and IOP, including dual-diagnosis support when mental health symptoms are part of the picture.
What outpatient care is not
Outpatient care is not passive. It isn't a few inspirational conversations while someone continues living in the same exact cycle. It only works when the program responds quickly to changes and the patient has enough external stability to use the support.
A good outpatient plan doesn't ask whether someone can white-knuckle recovery. It asks whether the structure around them is strong enough to carry them through the unstable parts.
That distinction matters in DFW because many adults want help that fits around jobs, children, classes, or family obligations. Flexible care can be a major advantage, but only if safety comes first and the program is prepared to increase support when warning signs show up.
How to Get Meth Detox Help in Dallas and Euless
It is 9 p.m., the person you love has not slept, their mood is getting darker, and everyone in the house is trying to guess whether tonight is manageable or whether it is turning into an emergency. That is usually the point when families need a clear plan, not more debate.

In Dallas, Euless, and the surrounding DFW area, the safest first move is a clinical assessment that looks at current meth use, psychiatric symptoms, sleep, safety, and the home environment. The goal is to decide what level of care fits the situation today. Some adults can begin with structured outpatient treatment. Others need inpatient or psychiatric stabilization first.
Start with the right questions
The first conversation should help answer practical concerns quickly:
- Is the person safe right now? Severe depression, suicidal thinking, paranoia, psychosis, or inability to stay safe changes the plan immediately.
- Can treatment address mental health at the same time? Meth withdrawal often overlaps with anxiety, trauma, depression, or thought disturbance.
- How much structure will the first week include? Ask how often the patient will be seen and who monitors changes in mood, sleep, and cravings.
- What happens if outpatient is not enough? A good program should explain its process for stepping someone up to a higher level of care without delay.
- How will payment and insurance be handled? Families need that answer early so they can act, not stall.
These questions matter because choosing care in DFW is often a real-world trade-off. Work schedules, children, transportation, and privacy concerns can make outpatient appealing. Safety still comes first.
Prepare for admission without overcomplicating it
If outpatient appears appropriate, keep the setup simple and honest. Bring a clear account of recent use, missed sleep, appetite changes, agitation, cravings, and any mental health symptoms. Leave out the polished version. Good decisions depend on accurate information.
Home support also needs to be realistic. Early recovery may require help with rides, meals, a quieter place to sleep, and reduced contact with people connected to meth use. If nobody at home can help monitor worsening symptoms, that matters in the placement decision.
Insurance verification is usually part of the admissions process, but benefits still have to be checked case by case. It also helps to think one step past detox. Once the acute crash starts to settle, some adults do better when they rebuild daily structure with sleep routines, meals, therapy, and basic physical activity. Later in recovery, resources such as fitness exercises for muscle growth can support that rebuilding phase, but they do not replace detox or clinical treatment.
For adults in Dallas and Euless, the best next step is a prompt assessment with a program that can evaluate safety, explain whether outpatient or inpatient makes more sense, and adjust the plan if symptoms worsen.
Your Next Step Is the Most Important One
A lot of families reach this point after a hard night. The person has crashed, slept for long stretches, become agitated, or said things that raise concern. Everyone wants one clear answer right away. What matters now is choosing the safest setting and getting an assessment before the situation shifts again.
Detox from methamphetamine gives the brain and body a chance to settle. Recovery takes more than the first few days. I often remind families that early improvement can be misleading. Someone may look calmer after sleep and food, yet still need close monitoring, psychiatric support, or a higher level of care once the full picture is clear.
For adults in Dallas-Fort Worth, the practical question is usually simple. Can this person be treated safely as an outpatient, with enough structure and support to get through the withdrawal period and into ongoing care? Strong outpatient treatment means more than a few check-ins. It should include a clear schedule, therapy, relapse-prevention planning, and dual-diagnosis support when depression, anxiety, paranoia, or other mental health symptoms are part of the case. Programs that offer PHP or IOP can provide that structure while allowing the person to stay connected to home, work, or family responsibilities when it is safe to do so.
Some people still need inpatient care first. That is not a failure. It is the right call when safety, supervision, or psychiatric stability cannot be managed at home.
The next goal is rebuilding daily function. Sleep, meals, hydration, therapy attendance, and reduced contact with people tied to meth use usually matter more than motivation speeches. Later, once a person is medically stable and clinically ready, simple physical routines can help restore consistency. Resources such as fitness exercises for muscle growth may fit into that later stage, but they do not replace detox, psychiatric care, or addiction treatment.
A qualified assessment changes the situation from guesswork to a plan.
Maverick Behavioral Health provides outpatient addiction and dual-diagnosis treatment for adults in Euless and the Dallas-Fort Worth area, including PHP, IOP, and standard outpatient care. Anyone who needs guidance on meth detox, level of care, or insurance verification can speak confidentially with the admissions team.