

Leaving treatment often feels strange in a way people don't expect. The structure is gone, the phone is back on, work texts start coming in, family wants updates, and familiar streets around Euless, Dallas, or Fort Worth can bring up old patterns fast. A person can be committed to recovery and still feel uneasy about what happens when real life starts moving again.
That's where a relapse prevention plan stops being paperwork and starts becoming protection. Relapse prevention became a formal clinical strategy in the late 1980s, shifting addiction care away from viewing relapse as simple “failure” and toward treating it as a predictable risk that can be reduced with structured planning, according to this NIH overview of relapse prevention. That shift matters because shame keeps people stuck, while planning gives them something concrete to do.
In early recovery, small things matter more than is commonly understood. Sleep gets off track. A drive past an old liquor store hits differently after a hard day. A family argument feels sharper. That's why practical routines belong in recovery from day one, and why a solid evidence-backed sleep guide can be useful for building steadier nights when the body and mind are still settling down.
Table of Contents
- Your Proactive Path to Lasting Recovery
- Identifying Your Personal Triggers and Warning Signs
- Building Your Action Plan Step by Step
- Integrating Professional Support for Stronger Results
- Creating Your Daily Recovery Environment
- Your First 90 Days and How to Get Help in Dallas-Fort Worth
Your Proactive Path to Lasting Recovery
A good plan starts with one mindset change. Relapse prevention strategies aren't built for people who expect to fail. They're built for people who want a clear response before stress, cravings, or old routines catch them off guard.
That matters in North Texas because recovery doesn't happen in a bubble. A person may leave a treatment setting and go straight back to traffic, financial pressure, family stress, social invitations, and neighborhoods linked to past use. Hoping motivation will carry the whole load usually doesn't work for long. Specific preparation works better.
Practical rule: Recovery gets stronger when a person plans for predictable risk instead of acting surprised by it.
The clinical model behind relapse prevention changed the conversation in addiction treatment. It framed relapse as something that often develops through identifiable risks and manageable decision points, not a sign that treatment “didn't work.” That gives people room to respond early, ask for help faster, and treat a difficult day as a signal to use the plan.
A strong plan also lowers the emotional temperature. Instead of asking, “What's wrong with me for feeling triggered?” the better question becomes, “What usually sets this off, and what will I do next?” That shift sounds small, but it changes behavior.
Three ideas usually help clients most at the beginning:
- Expect stress: Returning home, work, or family life can stir up urges even when recovery is going well.
- Plan in writing: Thoughts disappear under pressure. A written plan doesn't.
- Act early: The best time to interrupt a relapse process is before actual substance use.
That's the posture that makes the rest of this work useful. Calm, honest, and prepared.
Identifying Your Personal Triggers and Warning Signs
The first draft of a relapse prevention plan should be less about inspiration and more about accuracy. People don't need a perfect life story on paper. They need a usable map of what puts recovery at risk.
NIH-reviewed literature notes that relapse is often a gradual process with warning signs and stages before actual use, and plans that focus only on abstinence without tracking early signals miss the best window for intervention in this review of relapse dynamics. That means the work starts before a craving becomes overwhelming.
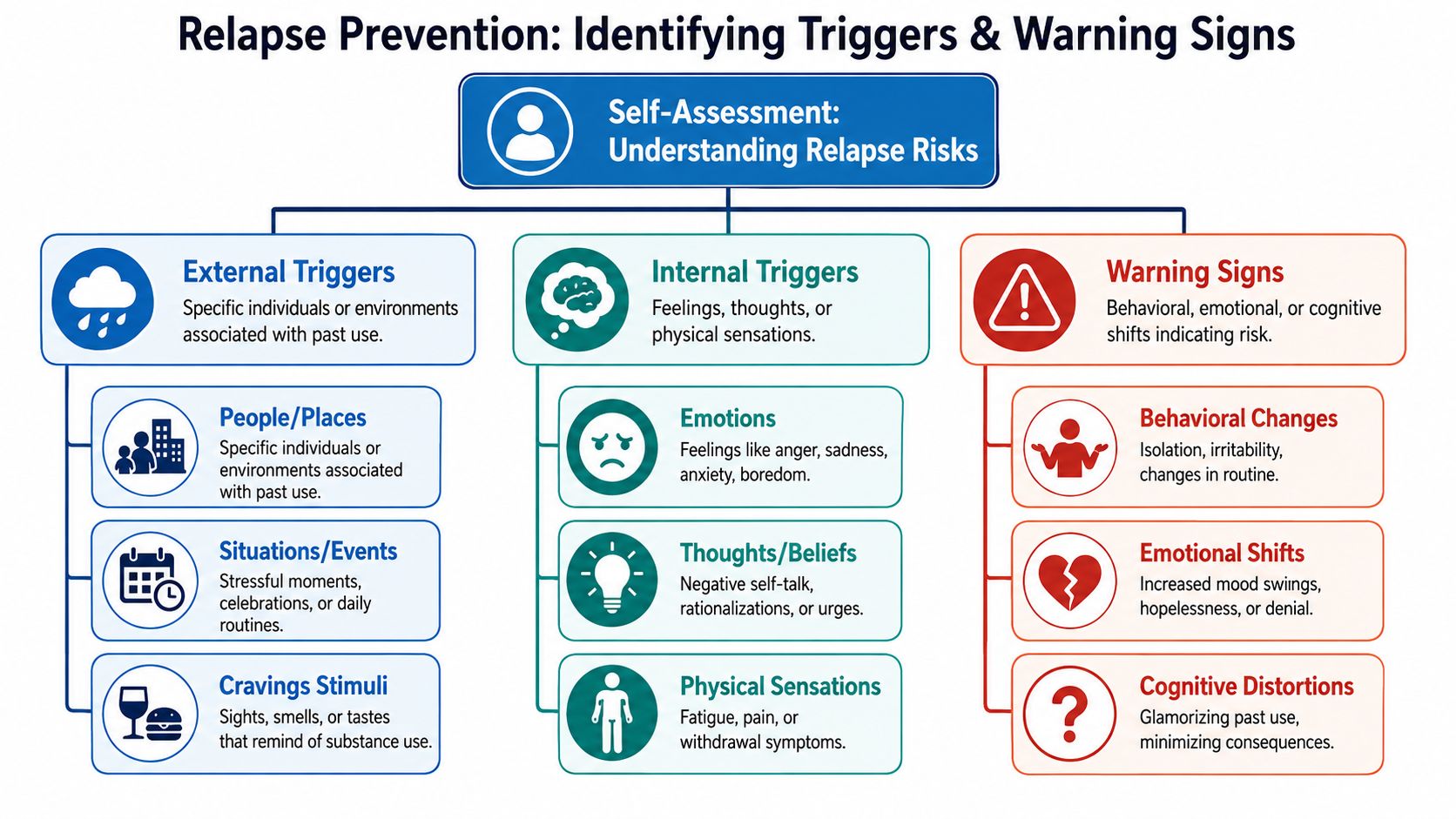
Internal triggers
Internal triggers are the states a person carries inside. They often look harmless at first because no one else can see them.
Common categories include:
- Emotions: anger, shame, loneliness, anxiety, boredom, grief
- Thought patterns: “I can handle just one,” “Nobody would know,” “I'm doing better, so maybe I don't need support”
- Physical states: exhaustion, body tension, poor sleep, pain, feeling restless, feeling keyed up
A useful exercise is to look back at prior use and ask a few direct questions:
- What feeling usually showed up first?
- What thought made use seem reasonable?
- What physical sensation made it harder to think clearly?
For one person in Euless, the trigger may be panic after work. For another, it may be boredom on a Sunday afternoon when the house is quiet. For someone else, it may be conflict with a partner followed by the urge to leave and disappear for a few hours. Different trigger, same need for a planned response.
External triggers
External triggers are easier to spot once a person starts naming them plainly. They include the people, places, routines, and events linked to past use.
A trigger list might include:
- People: old using friends, relatives who minimize recovery, people who contact only at night
- Places: a certain apartment complex, a parking lot, a bar district in Dallas, a gas station where alcohol was always bought
- Situations: payday, being alone in a hotel, sports events, family holidays, nights after arguments, long commutes
- Sensory cues: smells, music, seeing certain bottles, driving a familiar route
A trigger isn't proof that recovery is weak. It's information about where more structure is needed.
Many clients are surprised by how ordinary external triggers can be. The issue isn't only major crises. It can be getting off work early with no plan, scrolling a contact list, or taking the same route home that used to end in drinking or using.
Warning signs before a lapse
Warning signs are different from triggers. A trigger is a risk factor. A warning sign is evidence that the person is already drifting.
A short self-check can help:
| Warning area | What it may look like |
|---|---|
| Behavior | skipping meetings, isolating, staying out late, avoiding calls from safe people |
| Mood | irritability, hopelessness, numbness, sudden defensiveness |
| Thinking | romanticizing past use, minimizing consequences, resenting accountability |
| Routine | poor sleep, missed meals, no schedule, missed therapy, chaotic weekends |
A practical risk map should fit on one page. It should name the top internal triggers, the top external triggers, and the early warning signs that show the plan needs to be used immediately. If the list is too broad, it becomes hard to follow. If it's honest and specific, it becomes useful fast.
Building Your Action Plan Step by Step
A relapse prevention plan works when it answers one question clearly. When this happens, what will this person do next? General intentions don't hold up well under stress. Specific actions do.
A CBT-based relapse prevention plan typically starts by assessing substance use history, identifying internal and external triggers, and then creating an action plan that maps each high-risk situation to a coping response, support contact, or emergency step, as described in this relapse prevention planning overview.
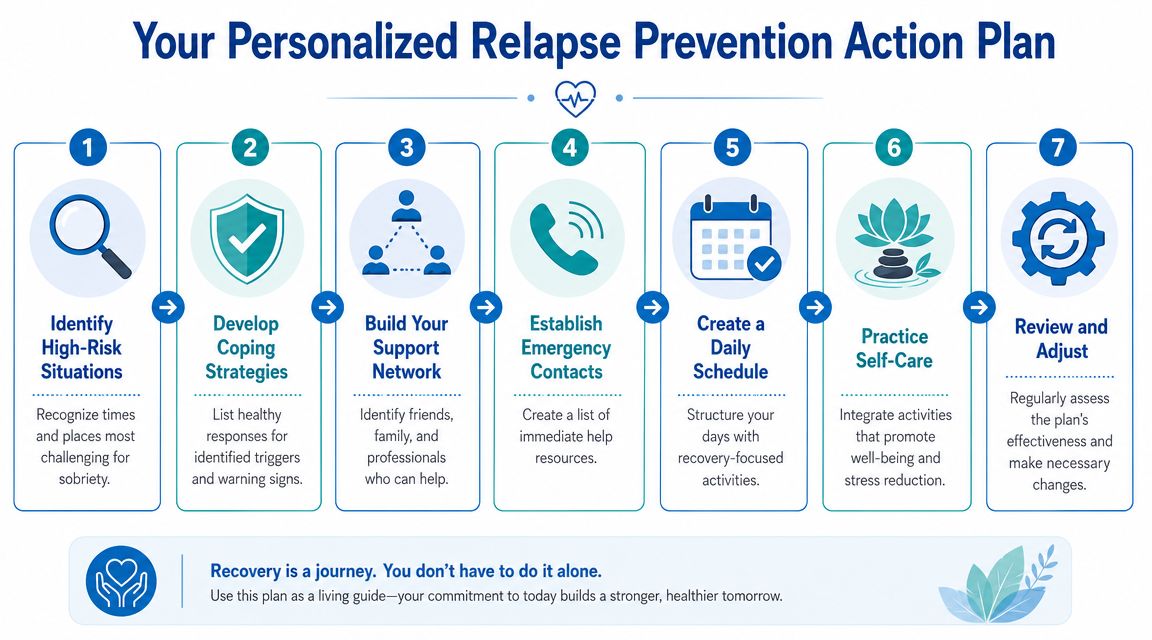
Start with a simple written format
The most practical format is a short worksheet or note on a phone that can also be printed. It should be easy to read when emotions are running high.
A workable layout looks like this:
- Trigger or high-risk situation
- Early warning sign
- Immediate coping action
- Who to contact
- Exit or emergency step
Here's a plain example:
| Trigger | Warning sign | Immediate action | Support contact | Emergency step |
|---|---|---|---|---|
| Leaving work stressed | racing thoughts, urge to isolate | sit in car, breathe, drink water, call support before driving | sponsor, therapist, sober friend | drive to meeting or safe home, not old neighborhood |
| Argument at home | anger, “I need out of here” thinking | take a walk, no texting old contacts, reset after 20 minutes | family-safe person, counselor | leave with safe person, go to public safe location |
| Weekend boredom | sleeping late, skipping plans | attend meeting, gym, coffee with sober peer | recovery peer | ask someone to stay connected through the afternoon |
People who need help building stronger day-to-day responses can also review practical coping skills for addiction recovery and fold the ones that fit into their written plan.
Match each trigger to one action
This is the part often skipped, and it's usually the part that makes the difference. Every major trigger needs a matched behavior, not just a promise to stay sober.
Examples of trigger-to-response matching:
- If loneliness hits at night, the response might be calling one safe person, attending an evening meeting, and not staying alone with a spiraling thought pattern.
- If an opioid craving starts after physical pain or stress, the response might be contacting the treatment team, using prescribed supports as directed, and avoiding any stop that puts access within reach.
- If alcohol cravings rise during work dinners or social events, the response might be driving separately, arriving late and leaving early, ordering a nonalcoholic drink immediately, and texting a support person before and after.
The plan should tell a person what to do in the first five minutes, not just what kind of person they want to be.
One strong method is to write each response in the first person when drafting it privately, even if the treatment team reviews it together. That makes the instruction feel immediate. Since this article is guiding from the outside, the key is still the same. Each high-risk moment needs a visible next step.
Add an emergency layer
Some situations need more than a coping skill. They need an escape route.
An emergency layer should cover:
- Where to go if the current place becomes unsafe
- Who to call first and who to call second
- What to remove such as cash access, contact with unsafe people, or idle driving time
- What to do after a lapse so one use doesn't become a full return to old behavior
A weak plan says, “Avoid triggers.” A stronger plan says, “If a cousin offers pills at a family gathering in Dallas, leave immediately, call support in the parking lot, and go straight to the next safe location already listed in the phone.”
That's what practical relapse prevention strategies look like. Not abstract advice. A set of rehearsed responses attached to real life.
Integrating Professional Support for Stronger Results
A written plan matters. On its own, it's often not enough. Recovery gets more stable when trained support helps test the plan, adjust it, and catch blind spots that a person or family may miss.
The strongest relapse prevention frameworks explicitly match triggers to responses by listing specific people, places, emotions, and thoughts that predict use, then assigning a concrete behavior such as cognitive reframing, urge surfing, or contacting support in this clinical summary of relapse prevention. That kind of work is easier to do well with professional guidance.

What professional support actually adds
Professional care doesn't replace personal responsibility. It gives that responsibility structure.
A counselor, physician, or outpatient team can help with several hard parts of recovery:
- Pattern recognition: identifying the triggers a client keeps minimizing
- Skill practice: rehearsing what to say, where to go, and how to interrupt cravings
- Accountability: noticing when sleep, mood, attendance, or isolation start slipping
- Medication support: for some people, including those with opioid dependence, MAT such as Suboxone can be an important part of reducing withdrawal and craving pressure
- Dual diagnosis care: when depression, anxiety, trauma, or another mental health condition is feeding substance use risk
A person leaving inpatient treatment in the Euless or Dallas area often needs more than a weekly check-in. If work stress is rising, family trust is shaky, and cravings are active, a higher step-down level of care may fit better than standard outpatient alone.
How outpatient care fits into daily life
Partial Hospitalization Programs and Intensive Outpatient Programs help bridge the gap between a controlled setting and independent living. They give people a place to practice real-world recovery while still having frequent support, clinical monitoring, and scheduled therapy.
For readers comparing levels of care, this guide to how IOP therapy works can clarify what that structure looks like during the week. In the Euless and greater Dallas-Fort Worth area, one local option is Maverick Behavioral Health, which provides PHP, IOP, standard outpatient care, dual diagnosis treatment, and MAT as part of individualized planning.
Motivation matters. But motivation without structure often loses to stress, fatigue, and access.
Families should hear this too. Support doesn't mean policing every move. It means helping create consistency. Rides to therapy, clear house rules, honest communication, and quick action when warning signs appear all strengthen the plan. The best support systems aren't dramatic. They're dependable.
Creating Your Daily Recovery Environment
Many lapses don't begin with a dramatic moment. They start with a day that has too much space, too little rest, and no clear recovery rhythm. That's why daily structure belongs in the same conversation as cravings and triggers.
Major recovery guidance notes that insomnia, fatigue, stress, and unstructured time can function as relapse triggers, and plans that fail to turn coping into observable routines leave people exposed to predictable high-risk states in this aftercare and relapse prevention guide.

A day with structure looks different
Consider two versions of the same Saturday in DFW.
In the first, a person sleeps late, skips breakfast, ignores texts from safe friends, starts driving with no destination, and ends up near places tied to past use. Nothing “big” happened, but the day became risky hour by hour.
In the second, that same person wakes up at a planned time, eats, attends a morning recovery meeting, spends midday with a sober family member, exercises in the afternoon, and keeps the evening simple. The urge may still appear, but it has less room to take over.
Recovery usually weakens in the gaps. Routine closes many of those gaps before cravings get louder.
A stable daily recovery environment often includes:
- Consistent sleep and wake times: not perfection, just steadiness
- Regular meals: hunger and blood sugar swings can intensify stress and irritability
- Physical movement: walking, gym time, stretching, or anything sustainable
- Scheduled support: therapy, group, meetings, or recovery check-ins placed on the calendar
- Protected downtime: quiet activities that don't pull a person toward risky places or people
The environment around recovery matters
Home and social life matter too. A person early in recovery may need to remove alcohol from the house, block certain contacts, stop attending some events, or tell family members that surprise visits and chaotic conflict aren't workable right now.
The strongest environments usually share a few features:
- Clear boundaries: no substance use in the home, no unsafe visitors, no “just stop by” contact from old using peers
- Visible reminders: meeting schedules, written goals, emergency contacts on the fridge or phone
- Sober connection: local peer support in Euless, Dallas, or nearby communities, plus regular contact with one or two dependable people
- Meaningful activity: work, classes, volunteering, hobbies, faith community, or family roles that restore purpose
A person doesn't need an ideal life to build a safer one. The job is to make daily relapse prevention strategies visible enough that they happen even on rough days.
Your First 90 Days and How to Get Help in Dallas-Fort Worth
The first stretch after treatment deserves extra attention because risk is concentrated early in recovery. Independent summaries report that about 40% to 60% of people with addiction relapse at some point, about 40% to 80% of patients treated for alcohol use disorders have at least one drink within the first year after treatment, and one widely cited estimate says 85% of relapses occur in the first 6 to 12 months after treatment, while long-term risk drops substantially, with about 15% after 5 years cited by one source in this relapse rates summary. Those numbers are why the first months shouldn't be left to guesswork.

How to use the plan during the first months
The best approach is simple. Review the plan every day, not only when something goes wrong. Keep it on the phone. Print it if needed. Update it when a new trigger shows up or when an old coping response stops working.
A practical first-90-days focus often includes:
- Daily review: read the trigger list and today's schedule each morning
- Weekly adjustment: revise the plan with a therapist, sponsor, or trusted recovery support
- Fast response to change: if sleep drops, meetings slip, or isolation grows, increase support right away
- Insurance and access checks: if coverage is unclear, reviewing Community Health Choice eligibility may help some Texas residents understand one part of the benefits picture before arranging care
People dealing with opioid misuse may also need a more specific treatment path. This local resource on opioid addiction treatment near Euless and Dallas can help clarify next steps for outpatient support and medication-assisted care.
Local help in Euless and Dallas
No one in the Dallas-Fort Worth area needs to build this alone. If the plan feels scattered, if cravings are getting stronger, or if the return home already feels unstable, getting help quickly is the smart move.
Call (888) 385-2051 to speak with a caring professional about outpatient treatment options, verify PPO insurance, and talk through what level of support fits right now. A clear plan, the right schedule, and steady clinical support can make the first 90 days far more manageable.
If relapse prevention needs more structure, Maverick Behavioral Health can help adults in Euless, Dallas, and the wider DFW area build a practical recovery plan through outpatient treatment, including PHP, IOP, standard outpatient care, dual diagnosis services, and MAT. Call (888) 385-2051 to discuss options, verify PPO insurance, and get help putting a real plan in place.