


Some people in Euless, Dallas, and the wider DFW area are reading about treatment after another hard night. They may be trying to get through work while hiding withdrawal. They may be watching a son, daughter, spouse, or parent promise to stop, then use again just to avoid getting sick. Families often feel confused by that cycle. It can look like a lack of effort from the outside, even when the person is exhausted and scared.
That cycle has a medical side as well as an emotional one. Opioid use changes how the brain responds to pain, stress, reward, and survival. Once that happens, cravings and withdrawal can dominate daily life. Medication assisted treatment, often called MAT, helps interrupt that pattern so recovery can become possible in real life, not just in theory.
The benefits of medication assisted treatment go far beyond “helping someone quit.” MAT can reduce overdose risk, lower the chance of dangerous medical crises, and make it easier for a person to function at home, at work, and in treatment. For many people, especially those who need outpatient care in the Dallas-Fort Worth area, MAT offers a practical way to stabilize first and rebuild second.
Table of Contents
- The Cycle of Addiction and a New Path Forward
- How Medication-Assisted Treatment Restores Brain Balance
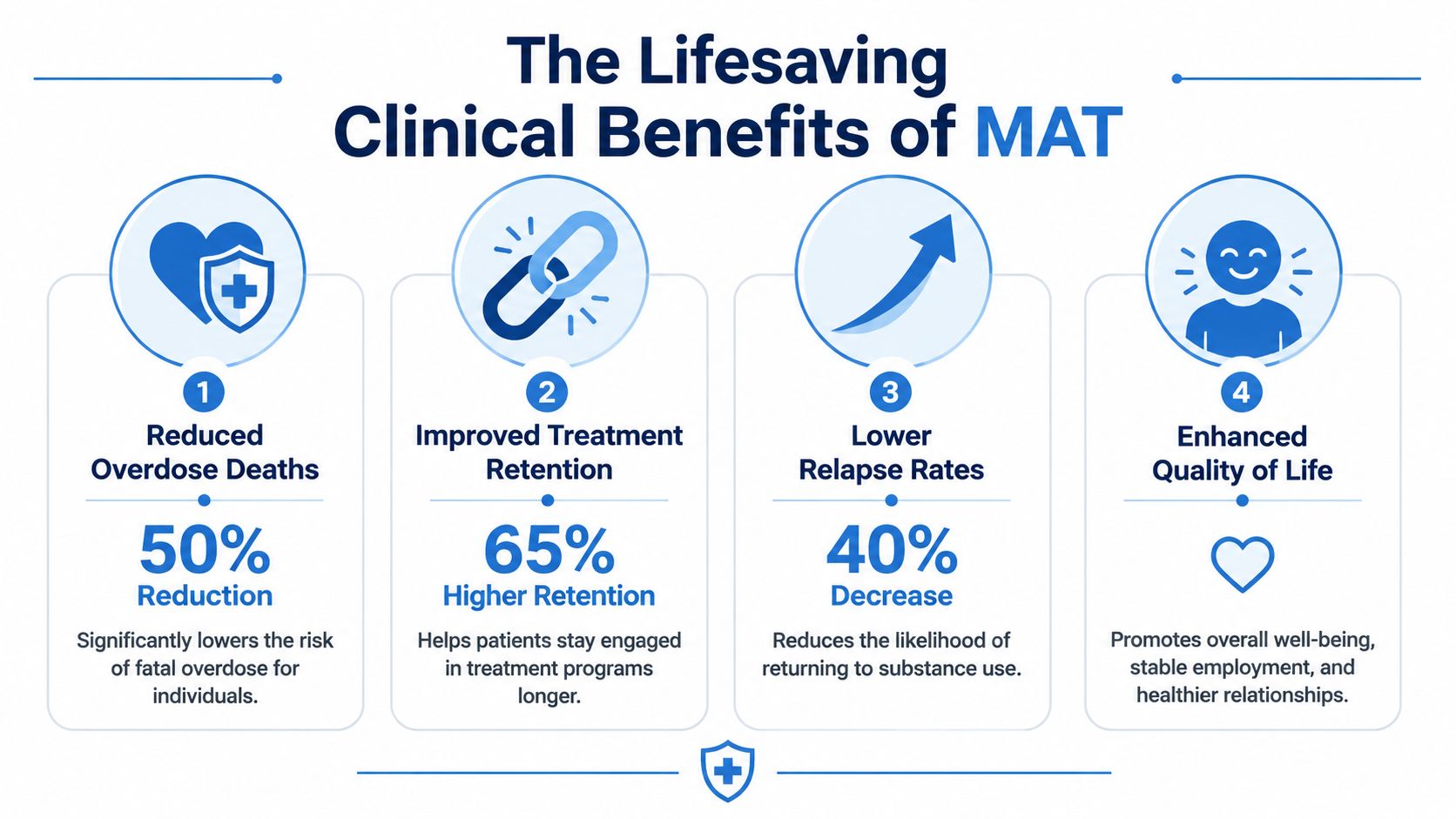
- The Lifesaving Clinical Benefits of MAT
- Comparing Common MAT Medications Like Suboxone
- How MAT Supports Whole-Person Recovery and Daily Life
- Starting MAT in the Dallas-Fort Worth Area
The Cycle of Addiction and a New Path Forward
A common pattern looks like this. Someone wakes up already feeling withdrawal. Before breakfast, the day is no longer about parenting, class, or work. It becomes about not getting sick. By afternoon, guilt sets in. By evening, promises are made again.
Families often respond with pressure, fear, or anger because the stakes are so high. The person using opioids may also want help and still feel unable to stop. That's one reason opioid addiction can feel so defeating. It overrides good intentions with physical distress and relentless craving.
MAT gives that person a different starting point. Instead of asking a dysregulated brain and body to recover through sheer willpower, it uses medication to reduce withdrawal and cravings while counseling addresses behavior, coping, stress, and relapse risk. In outpatient care, that can mean a person receives treatment while still living at home and continuing many normal responsibilities.
Recovery often begins when a person can get through an ordinary day without chasing relief from withdrawal.
That matters in practical ways. A person who sleeps through the night, shows up to appointments, eats regular meals, and can think clearly is in a much better position to do the hard work of recovery. MAT doesn't erase responsibility. It creates enough stability for responsibility to become realistic again.
Several day-to-day benefits often stand out early:
- Less time spent in crisis: The person isn't organizing the entire day around avoiding withdrawal.
- More mental space for treatment: Counseling becomes easier to engage in when the body is calmer.
- Safer outpatient recovery: Many people can begin healing without disappearing from family, school, or work.
- A more hopeful family dynamic: Loved ones often see steadier behavior before they hear perfect words.
For people across Euless and Dallas, that “new path” often starts with one simple shift in thinking. MAT isn't a shortcut. It's medical treatment for a dangerous condition. That difference helps many families move from suspicion to support.
How Medication-Assisted Treatment Restores Brain Balance
Some people hesitate because medication sounds like replacing one substance with another. That misunderstanding keeps families stuck. MAT is better understood as medical stabilization. A useful comparison is insulin for diabetes. The medication doesn't “cure” everything by itself, but it helps correct a biological problem so the person can function and follow a larger treatment plan.
Why withdrawal keeps pulling people back
With opioid addiction, the brain learns to expect opioids. When opioids drop out of the system, the body reacts with withdrawal. That can include physical discomfort, anxiety, agitation, and intense craving. In that state, many people aren't choosing between “good” and “bad” decisions in a calm way. They're trying to escape distress.
Buprenorphine helps because it acts on the same opioid receptors in a controlled way. According to clinical findings on buprenorphine in medication-assisted treatment, medications like buprenorphine are partial mu-opioid receptor agonists that normalize brain chemistry without producing a euphoric high. The same source notes that 60% of participants remained opioid-free during buprenorphine treatment, compared with 20% in control groups receiving no medication.
That kind of stabilization changes the daily experience of recovery. The person can wake up and think about getting to work on time, answering messages, or attending group therapy instead of spending the first hours of the day trying to stop withdrawal.
Why medication and therapy work better together
Medication handles one part of the problem. Therapy handles the rest.
A strong MAT plan usually includes several moving parts:
- Medication management: A clinician evaluates symptoms, response, side effects, and ongoing cravings.
- Individual therapy: The person works on triggers, shame, routines, and relapse patterns.
- Group support: Peers reduce isolation and help normalize the work of recovery.
- Behavioral skill-building: People practice how to manage stress, conflict, and high-risk situations.
Someone who wants a broader clinical overview can review what medication-assisted treatment involves.
Practical rule: Medication helps the brain settle down. Counseling helps the person decide what to do with that stability.
That combination is what makes outpatient treatment workable for many adults. It allows recovery to happen while the person remains connected to ordinary life. For people in DFW who need help without stepping away from every responsibility, that's often one of the most important benefits of medication assisted treatment.
The Lifesaving Clinical Benefits of MAT
A common scene in outpatient care looks like this. A family in Dallas-Fort Worth arrives exhausted after weeks or months of fear, sleeping lightly because every missed call could be bad news. The person seeking help often feels just as worn down. They are not asking for a lecture. They want to know one thing first. Will this treatment lower the chance of overdose and keep life from spinning into another medical crisis?
That is the clearest clinical benefit of MAT. It helps people stay alive long enough to build recovery.
Overdose prevention changes the whole picture
The highest-risk period in opioid use disorder is often the period when a person is trying, relapsing, cutting back, losing tolerance, and starting again. That pattern can make overdose more likely. Medications used in MAT reduce that danger by making the body and brain less likely to swing between extremes.
As the Substance Abuse and Mental Health Services Administration explains in its overview of medications for substance use disorders, FDA-approved medications are used to support recovery and reduce the risk of return to opioid use. That matters in real life, not only on paper. Fewer returns to uncontrolled opioid use generally means fewer overdose scares, fewer 911 calls, and fewer nights when a family is afraid to go to sleep.
In an outpatient MAT program, that protection starts to show up in everyday routines. A patient may come in for an evaluation, begin medication under clinical guidance, return for follow-up visits, and have the dose adjusted based on withdrawal symptoms, cravings, sedation, and function. The process works like setting a broken bone in a cast. You do not heal the whole body in one hour, but you create stability so healing can begin.
For readers who want a clearer picture of how that works in practice, outpatient medication-assisted treatment for opioid addiction explains how this level of care is used day to day.
Fewer medical emergencies mean recovery can stay on track
Another major clinical benefit is a drop in crisis-driven care. People who are caught in repeated opioid use often cycle through urgent care visits, emergency rooms, dehydration, infections, injuries, panic at home, and abrupt interruptions to work or parenting. Every crisis resets the clock.
MAT helps interrupt that pattern because it reduces the physical instability that keeps pulling people back into danger. The immediate goal is simple. Fewer emergencies. The long-term result is larger. A person has a better chance of showing up for counseling, keeping a job, making court dates, caring for children, and rebuilding trust one ordinary day at a time.
This is often what families notice first in DFW outpatient treatment. Life gets less chaotic. The person is more reachable. Appointments become more predictable. There is room to talk about sleep, appetite, transportation, stress, and relapse triggers because every week is no longer dominated by the next emergency.
A few clinical benefits stand out in that day-to-day experience:
- Lower overdose risk: Medication lowers the chance that a lapse turns into a fatal event.
- Less cycling between withdrawal and intoxication: Physical stability gives patients a safer starting point.
- Fewer crisis interruptions: Recovery work is easier to continue when ER visits and urgent setbacks are less frequent.
- More consistent follow-up: Outpatient visits, therapy, and medication checks can happen on a steadier schedule.
MAT gives recovery time to work. For many patients, that time is what saves their life.
Comparing Common MAT Medications Like Suboxone
People often ask one very practical question first. Which medication is being discussed?
That question matters because MAT isn't one single drug or one identical experience for every patient. A clinician considers opioid history, withdrawal status, motivation, relapse risk, schedule, and medical needs before recommending an option. In outpatient settings, two of the most familiar medications are buprenorphine and naltrexone.
Buprenorphine and Suboxone
Buprenorphine is a partial opioid agonist. In plain language, it attaches to opioid receptors in a controlled way and helps reduce cravings and withdrawal. It's commonly known through the brand name Suboxone when combined with naloxone.
For many patients, this option fits because it can help them stabilize while continuing normal life. Someone may still need counseling, structure, and close follow-up, but the medication can reduce the constant physical push to keep using. In everyday terms, people often describe this as finally being able to think straight enough to participate in recovery.
Buprenorphine may be a strong fit for a person who:
- Needs relief from withdrawal: Starting treatment is often easier when the body isn't fighting the process.
- Wants outpatient flexibility: Daily life can continue while the treatment team monitors progress.
- Has repeated relapse tied to cravings: Reduced craving can create a safer runway for therapy and routine.
Naltrexone and Vivitrol
Naltrexone works differently. It is an opioid antagonist, which means it blocks opioid effects rather than activating opioid receptors. A common brand form is Vivitrol, a monthly injection.
This approach may appeal to some people because it doesn't act like an opioid medication. But it also requires careful timing. A patient generally needs to be fully off opioids before starting, which can make the beginning of treatment more challenging for some individuals. That's one reason medication choice should always be personalized rather than driven by fear, stigma, or family pressure alone.
Naltrexone may be considered for someone who:
- Has already completed withdrawal: The person is past the stage where withdrawal management is the main need.
- Prefers a non-agonist option: Blocking effects may align better with personal preference or treatment goals.
- Benefits from a longer-acting format: A monthly injection can support consistency for some patients.
Comparison of Common MAT Medications
| Medication (Brand Name) | How It Works | Administration Method | Primary Benefit |
|---|---|---|---|
| Buprenorphine (Suboxone) | Partial opioid agonist that helps reduce withdrawal and cravings | Typically taken regularly in an outpatient setting | Helps stabilize the brain and body so the person can engage in recovery |
| Naltrexone (Vivitrol) | Opioid antagonist that blocks opioid effects | Often given as an injection on a scheduled basis | Supports relapse prevention for people who have already completed withdrawal |
Medication choice is rarely about which option sounds “stronger.” It's about fit. A patient with severe cravings and active withdrawal may need a different starting point than a patient who has already detoxed and wants a blocking medication.
The best MAT medication is the one that matches the person's actual clinical situation, not the one that sounds easiest to explain at dinner.
Families also get confused about time frame. Some patients stay on medication longer than they expected. That isn't failure. It may reflect what's safest and most stabilizing at that stage of recovery. The goal is not to rush. The goal is to build a recovery that can hold.
How MAT Supports Whole-Person Recovery and Daily Life
The benefits of medication assisted treatment become most real when daily life starts working again.
A person in early recovery may not be looking for abstract wellness. They may want to keep a job, make it to class, repair trust at home, or stop scaring their children. MAT can support those concrete goals because stability changes what a person can do between appointments.

Daily life gets more manageable
According to research on MAT and improved life stability, MAT significantly improves social functioning and stability. That research also notes that patients in MAT have higher treatment retention, which correlates directly with reduced criminal justice involvement and improved employment outcomes.
That kind of change often shows up in ordinary routines before it shows up in dramatic life milestones. A person starts answering the phone again. They become more predictable with money. They make it through a work shift without leaving in panic. A parent becomes more emotionally present at home.
Some of the most noticeable improvements include:
- Work and school consistency: A steadier body and mind make attendance and follow-through more realistic.
- Better family reliability: Loved ones often notice fewer disappearances, fewer broken promises, and less chaos.
- Safer decision-making: When cravings aren't driving the day, people can slow down and think.
- Stronger treatment engagement: Appointments become something the person can keep, not something they miss while chasing relief.
Dual diagnosis care matters
Many people with opioid addiction are also struggling with anxiety, depression, trauma symptoms, or other mental health concerns. When opioid use is active and withdrawal keeps hitting, it becomes very hard to sort out what belongs to addiction, what belongs to mental health, and what needs immediate treatment first.
MAT can help create enough stability for that work to happen. Once cravings and withdrawal settle, the person often has a better chance of participating in therapy, discussing symptoms truthfully, and tolerating the emotional work of recovery.
Outpatient care can be especially helpful in these situations. A patient can take what happens in therapy and use it the same week in real settings. That might mean practicing boundaries at home, handling stress at work differently, or learning how to respond to anxiety without using.
Some people don't need more lectures. They need enough stability to benefit from treatment.
Whole-person recovery means more than abstinence. It means building a life that becomes harder to abandon. MAT can support that process by helping the person stay physically steady while emotional, relational, and behavioral healing catches up.
Starting MAT in the Dallas-Fort Worth Area
Starting treatment is often the hardest step because people expect judgment, pressure, or a confusing intake process. Most are already carrying fear. They may worry about being seen, about missing work, about what medication means, or about whether they've “failed too many times” for treatment to help.
In the Dallas-Fort Worth area, outpatient MAT can offer a more manageable path. A person doesn't always need to disappear from daily life to begin getting better. They can enter care, complete an assessment, talk openly about opioid use, and work with a treatment team on a plan that fits the severity of the problem and the realities of everyday life.

What the first steps usually look like
Most outpatient MAT starts with a confidential clinical evaluation. The team asks about current opioid use, withdrawal symptoms, treatment history, mental health concerns, medical issues, and home responsibilities. From there, the provider recommends a level of care and whether medication is appropriate.
A typical beginning may include:
- Assessment and screening: The team gathers enough detail to recommend safe treatment.
- Medication planning: The provider explains options, timing, and what the first days may feel like.
- Therapy scheduling: Counseling and group support are built into the plan, not left as an afterthought.
- Ongoing adjustment: The plan changes as the patient stabilizes and progresses.
People searching locally can review opioid addiction treatment near Euless and the Dallas area to get a clearer sense of nearby outpatient options.
What families often need to hear
Families often want to know how to help without making things worse. A useful starting point is to focus on action rather than debate. Getting an assessment matters more than winning an argument about labels, blame, or motivation.
A few reminders can ease the first call:
- Treatment doesn't require perfect certainty: A person can be unsure and still take the next step.
- Medication decisions are clinical decisions: They should be made with a qualified provider, not social stigma.
- Outpatient care can fit real life: Many adults need a plan that works around family or job obligations.
- Early support matters: Waiting for “rock bottom” can expose the person to more danger.
The path forward doesn't have to start with a dramatic moment. It can start with a phone call, a screening, and a willingness to let trained professionals help decide what comes next.
People in Euless, Dallas, and across DFW who are looking for compassionate outpatient help can contact Maverick Behavioral Health to learn about MAT, Suboxone-based care, dual diagnosis treatment, and flexible outpatient options. A confidential conversation can clarify what level of care fits best and what starting treatment would look like. To speak with the admissions team, call (888) 385-2051.