


Most Intensive Outpatient Programs last 8 to 12 weeks, with attendance typically set at 3 to 5 days per week for 9 to 15 hours weekly. The exact timeline is personal, though, and it can range from 4 weeks to 6 months or more depending on symptom severity, relapse history, co-occurring mental health needs, and how steady progress looks in real life.
For many people in Euless, Dallas, and the wider DFW area, that question shows up at a stressful moment. They may be trying to keep a job, stay in school, manage family responsibilities, and decide whether treatment will take over their whole life. It won’t. A well-structured IOP is built for people who need serious support without stepping away from home, work, or class.
The better question isn’t just how long does iop last. It’s how long should this specific person stay in care to give recovery a real chance. That answer should be based on clinical needs, not wishful thinking, guilt, or a calendar.
Table of Contents
- The Standard IOP Schedule and Duration
- How IOP Compares to Other Levels of Care
- Key Factors That Personalize Your IOP Timeline
- Example IOP Timelines for Different Needs
- IOP for Working Professionals and Students in Dallas
- Get a Clear Timeline for Your Recovery Journey
The Standard IOP Schedule and Duration
Someone who needs treatment but still has to clock in for work tomorrow usually needs a simple answer first. Here it is. IOP is designed to deliver meaningful structure without requiring an overnight stay.
According to this overview of standard IOP duration, Intensive Outpatient Programs typically last 8 to 12 weeks, with 9 to 15 hours per week across 3 to 5 days. That setup gives people enough therapeutic contact to build momentum while still living at home and handling work, school, or family obligations.
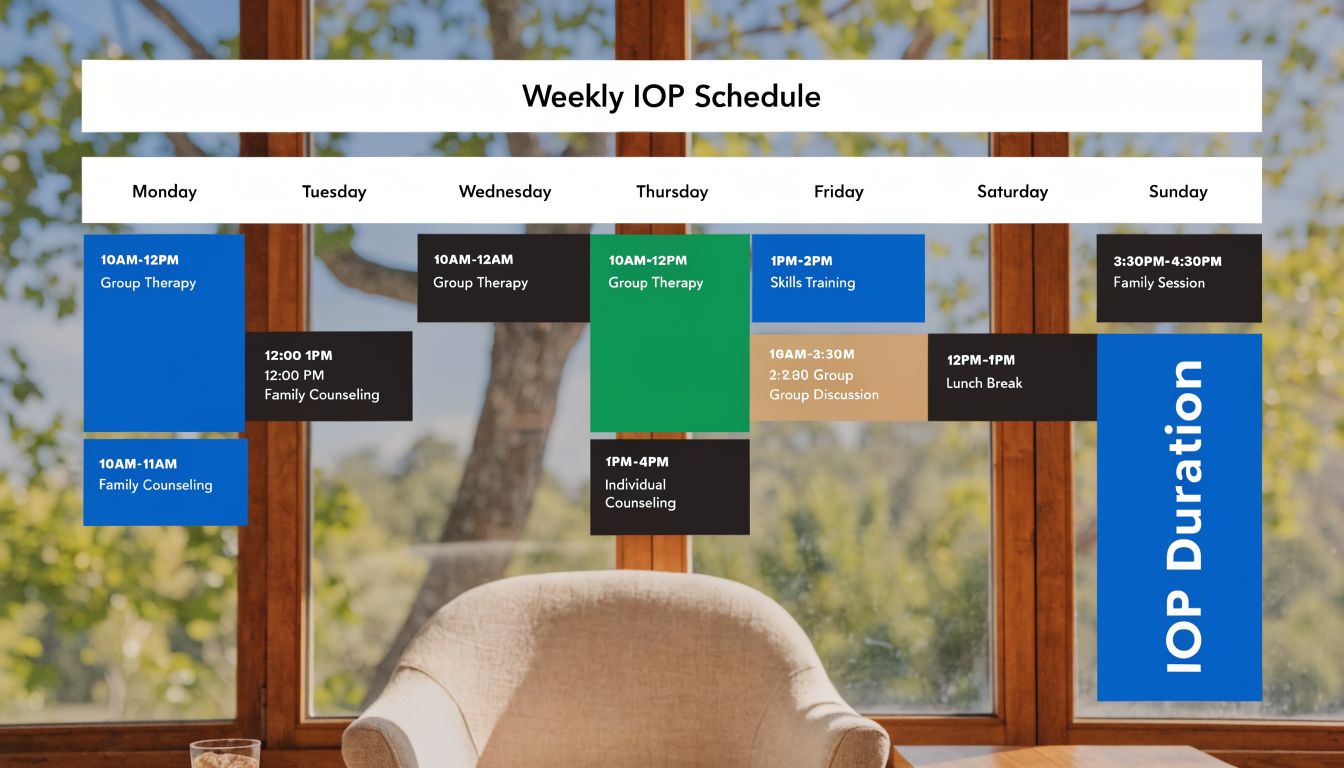
What a typical week looks like
A standard IOP week usually includes several therapy blocks spread across the week rather than one long session. That matters because recovery isn’t built in a single appointment. It’s built through repetition, accountability, and enough support between real-life stressors.
A typical structure may include:
- Group therapy days: Most of the weekly hours are often spent in therapist-led groups focused on relapse prevention, emotional regulation, and practical coping skills.
- Individual sessions: These help address personal triggers, treatment goals, and barriers that don’t always come up in a group setting.
- Skill-building work: Clients may practice communication, cravings management, boundary setting, or planning for high-risk situations.
People who are still learning what IOP therapy includes day to day often feel less overwhelmed once they see the schedule in concrete terms. It’s structured, but it’s still livable.
Practical rule: If a program feels so light that it barely disrupts old patterns, it may not be intensive enough for early recovery.
Why this format works
IOP sits in the middle ground. It’s more involved than weekly counseling, but it doesn’t pull someone fully out of daily life. That’s the point.
Living at home during treatment gives clients a chance to practice new skills where real triggers happen. They can attend sessions, go back to work or class, deal with family stress, and return to treatment with fresh material to process. That feedback loop is one reason IOP works well for people who are stable enough to stay safe outside a residential setting.
For most adults, 8 to 12 weeks is the right starting expectation. It’s long enough to create rhythm and short enough to feel manageable. But it should never be treated like a fixed contract. A calendar doesn’t determine readiness. Clinical progress does.
How IOP Compares to Other Levels of Care
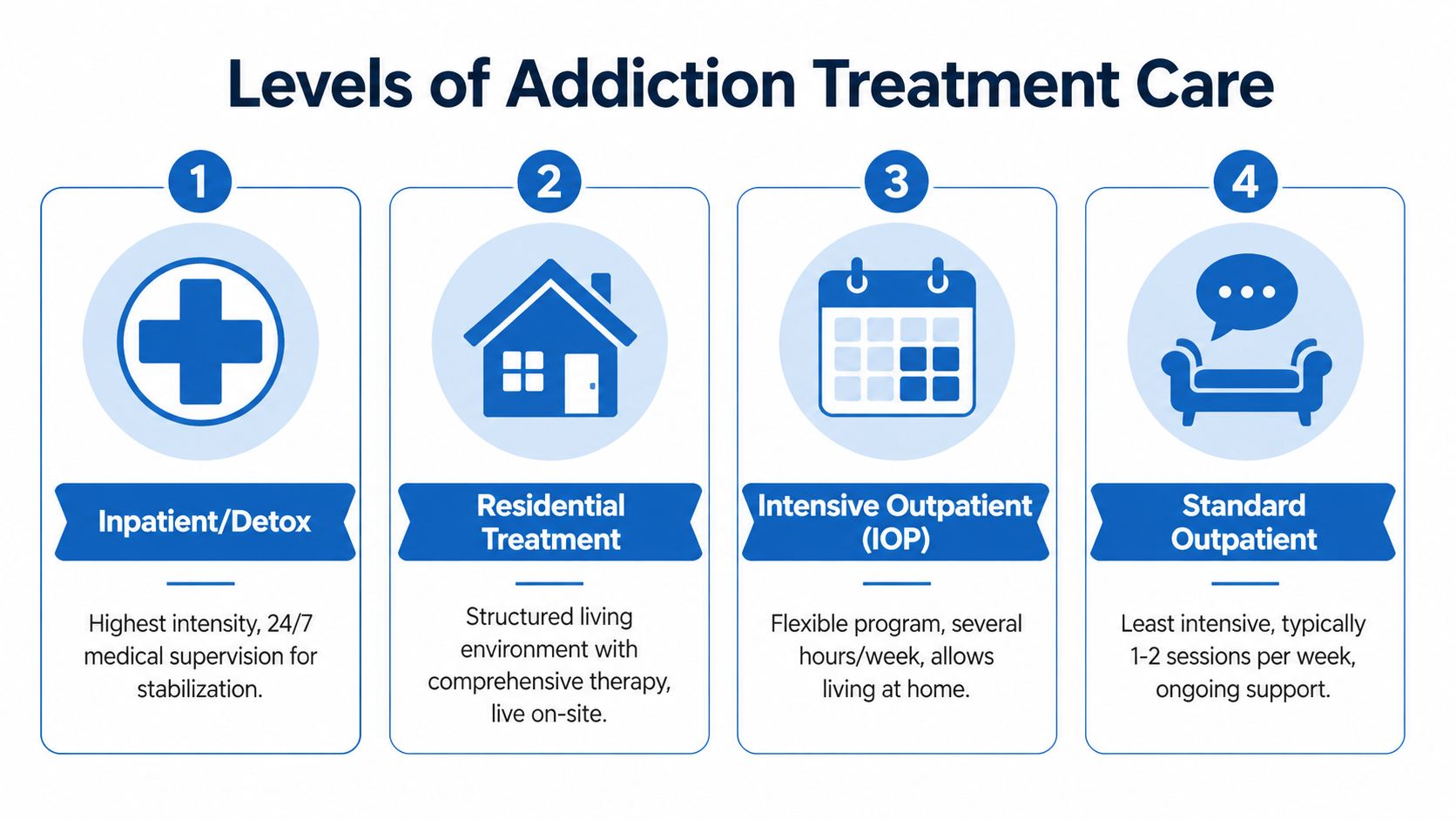
A lot of confusion comes from people hearing several treatment terms at once. Inpatient. Residential. PHP. IOP. Outpatient. They sound similar, but they solve different problems.
The cleanest way to understand IOP is to place it in the full treatment continuum. It’s not the most intensive option, and it’s not the lightest. It’s the level that fits people who need substantial support while still functioning safely outside a facility.
Where IOP fits
People considering IOP should think in terms of structure, supervision, and independence.
- Residential or inpatient care: Best for people who need round-the-clock monitoring, medical oversight, or complete removal from a dangerous environment.
- PHP: A strong step-down option from residential care, or a step-up for someone who needs daily treatment but can still return home at night.
- IOP: Appropriate for someone who needs frequent therapy and accountability but can safely live at home.
- Standard outpatient: Best for ongoing maintenance, lower-acuity needs, or continued support after more intensive treatment.
Someone deciding between levels of care may also want a broader breakdown of the difference between inpatient and outpatient treatment, especially when the main concern is how much daily life will need to change.
The right level of care should feel appropriately demanding. If it feels too easy, it may not be enough. If it feels impossible to sustain, it may be the wrong fit.
Treatment Levels at a Glance IOP vs. Other Programs
| Level of Care | Weekly Time Commitment | Living Situation | Best For |
|---|---|---|---|
| Residential or Inpatient | Highest level, full-time care | On-site | People who need constant supervision or stabilization |
| PHP | High, often near-daily treatment | Usually at home at night | People leaving residential care or needing more daily structure |
| IOP | Several treatment sessions each week | At home | People who need strong support without 24-hour supervision |
| Standard Outpatient | Lightest schedule | At home | People in ongoing recovery maintenance or lower-acuity care |
This comparison matters because people often ask how long does iop last when the deeper issue is whether IOP is the right starting point at all. If someone is actively unsafe, medically unstable, or unable to stay sober outside a controlled setting, IOP may be too low. If someone only needs occasional therapy, IOP may be more than necessary.
The best use of IOP is as a focused middle path. It gives enough repetition to interrupt destructive patterns, but it still lets clients build recovery in the environment where they live.
Key Factors That Personalize Your IOP Timeline
Two people can enter treatment on the same day and finish on very different timelines for good reason. One may stabilize quickly and step down sooner. Another may need a longer runway because the clinical picture is more layered.
That difference isn’t a failure. It’s the whole point of individualized treatment.

Clinical factors that stretch or shorten care
The first factor is the substance itself and the pattern of use. Alcohol, opioids, stimulants, and prescription misuse don’t play out the same way in the brain or in daily behavior. A person coming in after a brief relapse may need a very different timeline than someone with a long history of compulsive use.
The second factor is co-occurring mental health. Anxiety, depression, trauma, and mood instability can drive relapse if they aren’t treated alongside substance use. When both conditions are active, treatment often needs more time because the goal isn’t just stopping use. The goal is building stability that lasts.
Other factors matter too:
- Severity of symptoms: Longer addiction histories and repeated relapses often require more structure.
- Home environment: A supportive home can help someone progress faster. A chaotic one can slow progress.
- Engagement in treatment: People who attend consistently and use the skills between sessions usually move through care more effectively.
- Step-down status: Someone entering IOP after residential treatment may need less time than someone starting fresh in outpatient care.
Why the 90 day mark matters
According to SAMHSA-based guidance on IOP length and relapse risk, shorter programs under 90 days correlate with higher relapse rates because they may not give the brain’s reward system enough time to adjust. That same guidance notes that extended IOPs of 12 weeks or more can improve long-term outcomes, especially for people with dual diagnosis needs.
That matters because families often want a quick answer and a short finish line. Clinically, quick isn’t always smart.
Recovery has to last longer than the crisis that pushed someone into treatment.
A longer IOP timeline can be the right call when someone is finally doing the deeper work. Extending care isn’t a punishment. It’s often the first sign that treatment is being taken seriously enough to protect long-term sobriety instead of just achieving short-term compliance.
Example IOP Timelines for Different Needs
Abstract rules help, but understanding treatment length often benefits from real-world patterns. The timelines below aren’t promises. They’re practical examples of how care may unfold based on different clinical needs.
A shorter track after higher care
A person who has already completed detox, residential care, or PHP may enter IOP with a strong foundation. They may already have initial sobriety, medication stabilization, and a basic relapse prevention plan.
In that situation, an IOP timeline may fall closer to the shorter end. A program in the 4 to 6 week range can make sense when symptoms are mild, support at home is solid, and the primary goal is reinforcing gains made in a higher level of care. The focus is usually on transition, consistency, and preventing the slide back into old routines.
That shorter course only works when the basics are already in place. It shouldn’t be used to rush someone out.
A longer track for opioid use and MAT
Opioid recovery often needs more time, not less. Cravings, relapse risk, and the emotional fallout of opioid use can outlast the initial crisis period. That’s why medication-assisted treatment can be so important.
According to this review of longer IOP timelines for complex cases, extended IOPs can last from 12 weeks to over 6 months for opioid dependence with MAT or co-occurring mental health disorders. The same source states that a 90-day minimum produces the best results and cites findings that about 3 months of IOP can restore 60 to 70% of executive function in the prefrontal cortex.
That has real implications for planning. Someone receiving Suboxone support for opioid dependence may begin with a heavier schedule, stay in IOP for a longer stretch, and taper only after cravings, routines, and judgment become more stable.
A person taking medication for opioid recovery doesn’t need less therapy. They often do better with medication plus enough time in therapy to rebuild decision-making and daily structure.
A dual diagnosis timeline
Now consider someone dealing with cocaine use and anxiety, or alcohol misuse and depression. Early progress may look uneven. Substance use may improve first while sleep, panic symptoms, or emotional regulation lag behind. That’s normal.
A dual diagnosis IOP often lands in the longer range because treatment has two jobs. It has to reduce substance use and treat the mental health symptoms that fuel it. If the program ends too early, the underlying distress may pull the person back into self-medication.
A possible pattern might look like this:
- Early phase: Several treatment days each week focused on stabilization, honesty, and immediate coping tools.
- Middle phase: More consistent participation, better insight, and active work on triggers, relationships, and emotional regulation.
- Step-down phase: Gradual reduction in hours as the client demonstrates follow-through outside treatment.
These examples point to one clear truth. Asking how long does iop last only gets a useful answer when the question includes the person’s actual diagnosis, relapse history, support system, and day-to-day responsibilities.
IOP for Working Professionals and Students in Dallas
For people in Dallas-Fort Worth, scheduling is often the deciding factor. They’re not just asking whether treatment works. They’re asking whether treatment can fit around a real life that still includes a paycheck, classes, deadlines, and family expectations.
That concern is legitimate. If treatment requires someone to abandon every responsibility overnight, many people won’t start. Others will start and drop out fast. Flexible scheduling solves a practical problem, and it can also improve outcomes.

Why flexible scheduling changes outcomes
According to this Texas-focused report on flexible IOP scheduling, a 2025 ASAM analysis found that access to evening schedules reduced program dropout by 35%. That same source states that Texas Senate Bill 1234, effective January 2026, strengthens insurance coverage for flexible IOP schedules, improving access for working clients.
This is more than a convenience issue. It’s a retention issue.
When treatment is offered in the evening, a working adult doesn’t have to choose between getting help and keeping a job. A college student doesn’t have to disappear from class. A parent doesn’t have to create impossible daytime logistics every week. More people can stay in care long enough to benefit from it.
People seeking local options can review an intensive outpatient program in Dallas and Dallas County when they need a schedule that fits around normal responsibilities instead of replacing them.
What this means for people in Euless and DFW
In the DFW area, flexibility often changes both the feel and the function of treatment.
- Working professionals: Evening care can preserve employment while still creating a firm recovery routine.
- Students: Class schedules and treatment can coexist, which lowers the pressure to delay help until things get worse.
- Parents and caregivers: Predictable scheduling makes attendance more realistic when family obligations are nonnegotiable.
A rigid schedule can make a reasonable program feel impossible. A flexible schedule can make the same level of care sustainable. That matters because treatment only works when people can keep showing up.
The practical recommendation is simple. Anyone balancing work or school in Dallas, Euless, or nearby communities should ask about session timing first. Not last. If the schedule doesn’t fit, even a strong clinical program can become hard to complete.
Get a Clear Timeline for Your Recovery Journey
The most useful answer to how long does iop last is also the most honest one. Typically, individuals should expect 8 to 12 weeks as a starting frame, but the right timeline depends on what will genuinely support lasting recovery. Some people need a shorter step-down period. Others need a longer stretch because the addiction is more severe, the relapse pattern is chronic, or mental health symptoms are still active.
The mistake is treating treatment length like a personal preference. It’s a clinical decision. The target isn’t finishing fast. The target is leaving with enough stability, insight, and practice to keep going after formal treatment ends.
The right question to ask admissions
A strong admissions conversation should help clarify more than just the calendar. It should identify what level of care fits, what barriers could interfere with attendance, and what would make completion realistic.
The most important questions are usually these:
- How much structure is needed right now: Someone leaving a higher level of care may need reinforcement. Someone entering treatment in crisis may need more support before IOP is enough.
- What could interrupt completion: Work conflict, transportation, unstable housing, and untreated anxiety all affect how long care should last.
- What happens after IOP: Good treatment planning includes step-down care, relapse prevention, and a realistic aftercare path.
According to this treatment outcome summary on completing the full recommended IOP course, people who complete the full clinically recommended course of IOP are significantly more likely to maintain sobriety at the one-year mark than those who leave early. The same source states that completing the program, regardless of its specific length, is the single biggest predictor of long-term success.
That point deserves attention. People often fixate on whether treatment will be too long. They should be asking whether they’ll stay long enough to make it work.
Finishing the right plan matters more than finishing a short plan.
What to do next
For someone in Euless or the Dallas area, the next step should be straightforward. Get assessed. Get a real recommendation. Don’t guess based on internet averages alone.
A good admissions team should be able to help with:
- Level-of-care screening: Determining whether IOP is appropriate or whether a higher or lower level makes more sense.
- Schedule planning: Matching treatment times to work, school, or family demands.
- Insurance review: Clarifying benefits and reducing uncertainty around cost, especially for people with PPO coverage.
- Timeline expectations: Giving a realistic estimate based on substance use history, mental health needs, and current stability.
People delay treatment when the process feels vague. It gets easier when the next move is specific. A confidential phone call can answer the practical questions fast and remove a lot of fear.
Maverick Behavioral Health helps adults in Euless and the Dallas-Fort Worth area find the right level of outpatient care without guesswork. For a free, confidential conversation about IOP length, scheduling, insurance, and what treatment could look like in real life, call (888) 385-2051. The call doesn’t commit anyone to enroll. It gives them a clear answer and a practical next step.