


Some readers land on a page like this after another bad morning. They woke up anxious, replayed what happened the night before, promised themselves it wouldn’t happen again, then found themselves searching for how to stop drinking alcohol before the day even started. Others have been functioning for a long time, holding a job, paying bills, showing up for family, while recognizing that alcohol now runs more of life than they want to admit.
Both situations are common. Neither means a person has failed. It usually means the problem has reached the point where vague advice like “just cut back” or “use more willpower” isn’t enough.
A safer path starts with honesty about two things. First, quitting can be emotionally hard even for someone who isn’t physically dependent. Second, for some people, stopping suddenly can be medically dangerous. That difference matters. A person in Euless, Dallas, or anywhere in DFW deserves guidance that treats both the emotional side and the safety side seriously.
This guide is built for that moment. It gives a practical way to prepare, a clear warning about withdrawal risk, and a realistic picture of what treatment and long-term recovery can look like close to home.
Table of Contents
- Your First Step Starts with a Plan to Stop Drinking
- Preparing Your Mind and Environment to Quit Alcohol
- Understanding and Safely Managing Alcohol Withdrawal
- Finding the Right Alcohol Treatment Program in Dallas
- Building a Sober Life with New Coping Skills
- Your Aftercare Plan for Long-Term Relapse Prevention
Your First Step Starts with a Plan to Stop Drinking
A person usually doesn’t search for help by accident. They might be sitting in a parked car before work, staring at the steering wheel and thinking, “This has gone too far.” They might be hiding how much they drink from a partner, or noticing that every plan, every stress response, and every social event now seems to involve alcohol.
That moment matters because it’s often the first clear sign that denial is cracking. Recovery tends to start there, not when life is completely destroyed, but when someone becomes willing to admit that alcohol is taking more than it’s giving.

Many people wait because they think they need to feel more certain. They don’t. The first step is often less dramatic than expected. It can be telling one trusted person. It can be choosing not to keep alcohol in the house tonight. It can be reading about the first step in recovery and recognizing that change usually begins with a simple decision to stop pretending things are under control.
What a real plan looks like
A useful plan is concrete. It answers a few direct questions:
- When will drinking stop or pause
- What risks are present
- Who will know about the plan
- What support will be used if cravings hit
- What happens if withdrawal starts
The people who make progress aren’t always the most motivated at the start. They’re often the ones who stop keeping recovery vague.
There’s also good news here. A person doesn’t need to solve the next year today. They only need a starting point that’s honest, safe, and specific enough to carry them through the first stretch.
Hope matters, but structure matters more
Motivation rises and falls. Stress happens. Shame shows up. Social pressure doesn’t disappear because someone made a private promise on a hard day. That’s why a plan works better than a feeling.
The goal isn’t perfection. The goal is to move from fear and secrecy into action. For some people that action starts at home with preparation. For others, especially heavy or long-term drinkers, it starts with a professional assessment before they stop at all.
Preparing Your Mind and Environment to Quit Alcohol
Quitting goes better when the decision is made before the next craving, the next argument, or the next invitation out. Waiting until temptation is in the room usually leads to negotiating with it. Preparation reduces that problem.
One practical model is a time-limited challenge. A study on a structured 30-day alcohol abstinence challenge found a 67.6% success rate in completing full abstinence among heavy drinkers, and 85.3% reported health benefits even when they didn’t do it perfectly. That matters because many people quit after one slip, when the better move is to keep going with more structure.
Choose a quit date that means something
Some people do best with a start date in the next few days. Too much delay creates room for rationalizing. Others need a little time to arrange support, work obligations, childcare, or a medical consult if dependence is likely.
A quit date should be intentional, not symbolic only. “Monday” is fine. “After this work trip” is fine. “As soon as the alcohol in the house is gone” usually isn’t a plan. It’s a delay.
Prepare the environment before the cravings start
A home can either support sobriety or constantly challenge it. The same is true for a car, office, gym bag, or garage fridge.
Consider this checklist:
- Remove alcohol completely: Clear out bottles, mixers, flasks, bar tools, and the backup stash people often keep “just in case.”
- Change the routine cues: If pouring a drink starts right after getting home, replace that window with another action such as a meal, a walk, a shower, or a call to someone supportive.
- Stock alternatives that are easy: Keep simple nonalcoholic options available so the hand-to-mouth habit doesn’t automatically pull a person back toward drinking.
- Clean up reminders: Glassware on display, drinking accessories, and event invites tied to heavy drinking can all become stronger triggers than people expect.
Practical rule: If alcohol is close by, easy to hide, and part of the normal evening routine, quitting becomes harder than it needs to be.
Tell the right people, not everyone
Accountability helps, but it works best when it’s selective. A person usually needs one or two people who can respond well under pressure, not a broad announcement that creates more stress.
Good support sounds like this:
- Someone who answers calls: especially in the evening or on weekends
- Someone who won’t minimize the problem: “Just have one” isn’t support
- Someone who can help with logistics: rides, childcare, covering a social plan, or staying nearby if things feel shaky
Identify what actually triggers drinking
Triggers usually fall into a few categories. Some are external, such as certain friends, bars, restaurants, work events, or the drive home. Others are internal, such as anger, loneliness, boredom, shame, or anxiety after a hard day.
A short written list helps. It doesn’t need to be polished. It only needs to be honest. If a person drinks every time conflict happens at home, that’s a trigger. If they drink the most on nights when they feel flat and exhausted, that’s a trigger too.
Build a response before the urge arrives
Cravings feel urgent when there’s no alternate plan. They become more manageable when the next step is already decided.
Useful responses might include:
- Delay the decision for a short period and leave the trigger setting.
- Text or call one person who already knows the plan.
- Eat something and hydrate if the urge is hitting during a low-energy window.
- Go somewhere incompatible with drinking for a while, especially during the usual drinking hours.
Preparation doesn’t make quitting easy. It makes it possible.
Understanding and Safely Managing Alcohol Withdrawal
This is the part many online articles handle too lightly. Some people can stop drinking and feel uncomfortable. Others can stop drinking and become medically unstable. Those are not the same situation, and guessing wrong can be dangerous.
People who drink heavily or have been drinking for a long time should not assume they can safely quit cold turkey at home. A 2025 CDC update discussed in the referenced clinical material noted a 15% rise in alcohol-related ER visits for unsupervised withdrawal in Texas, and outpatient programs that combine therapy and medication were reported to reduce severe withdrawal episodes by 60% compared with self-managed attempts. For many people in Dallas-Fort Worth, the safest first move is assessment, not bravado.
What mild symptoms can look like
Withdrawal doesn’t always begin dramatically. It may start with anxiety, sweating, shakiness, nausea, trouble sleeping, restlessness, or a racing heartbeat. People often dismiss these signs because they still feel functional.
The problem is that early symptoms don’t reliably predict what comes next. Someone may tell themselves it’s “just nerves” when the body is already showing dependence.
When symptoms become dangerous
Severe withdrawal can include seizures and delirium tremens, which is a medical emergency. If a person becomes severely confused, starts seeing or hearing things, or has a seizure after cutting down or stopping alcohol, they need emergency help.
The risk is higher when a person has a history of heavy daily drinking, prior withdrawal problems, or repeated quit attempts followed by relapse. In such cases, self-management can move from uncomfortable to unsafe very quickly.
| Symptom Severity | Common Signs | Recommended Action |
|---|---|---|
| Mild | Anxiety, sweating, nausea, insomnia, mild shaking | Contact a medical professional promptly for guidance before symptoms escalate |
| Moderate | Worsening tremors, marked agitation, vomiting, rising distress, inability to rest | Seek same-day clinical assessment and don’t stay alone |
| Severe | Seizures, severe confusion, hallucinations, signs consistent with delirium tremens | Get emergency medical help immediately |
A person doesn’t need to “wait and see” whether alcohol withdrawal gets worse if dependence is already likely. Safety decisions should happen early.
Who should be especially cautious
A person should pause before trying to quit alone if any of these sound familiar:
- Heavy and regular drinking: especially when alcohol has become part of daily functioning
- Morning drinking or drinking to steady nerves: a common sign of physical dependence
- Past withdrawal symptoms: shaking, sweating, panic, or insomnia after cutting back
- Multiple failed attempts: especially when each attempt becomes harder
- Co-occurring mental health symptoms: anxiety, depression, or panic can intensify the process
Why outpatient support can be the right level of care
Not everyone needs inpatient treatment. Some people need medical oversight, medication support, therapy, and daily structure while still living at home and continuing parts of work or family life. That’s where outpatient care can fit well.
For readers comparing levels of care, this overview of the difference between inpatient and outpatient treatment can help clarify what level of support may match the situation. In the Dallas and Euless area, outpatient detox support, medication-assisted treatment, and structured day programs can give people a safer way to stop without trying to muscle through withdrawal alone.
What to do today if withdrawal risk is possible
The safest immediate steps are simple:
- Don’t promise a same-day cold turkey quit without a medical assessment if dependence is likely.
- Tell someone nearby what’s happening so the person isn’t isolated if symptoms worsen.
- Call for a confidential assessment if there’s any doubt about withdrawal risk.
A person who’s unsure whether they can stop safely shouldn’t guess. They should call (888) 385-2051 for a free, confidential assessment and get clear guidance before symptoms escalate.
Finding the Right Alcohol Treatment Program in Dallas
Once withdrawal risk is addressed, the next question is practical. What kind of treatment fits real life? Many adults in Euless and the wider Dallas-Fort Worth area can’t disappear from work, school, parenting, or caregiving responsibilities for an extended period. That doesn’t mean treatment is out of reach. It means the level of care has to match both the clinical need and the person’s daily reality.
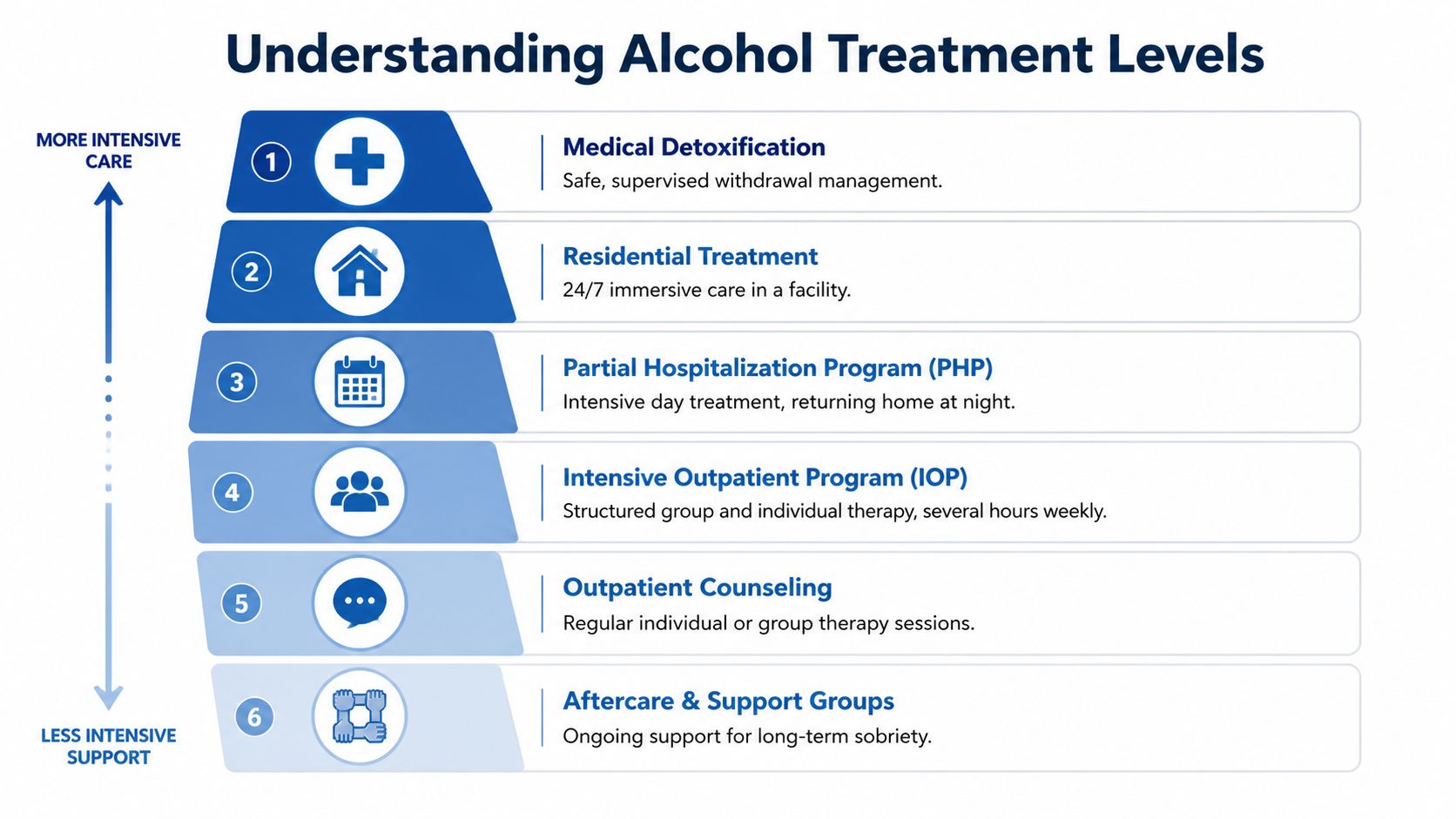
How to think about levels of care
Some people need a highly structured start. Others need support that wraps around a functioning schedule. The right program is the one that’s intensive enough to stabilize progress without being so mismatched that the person drops out.
A simple way to look at it:
- PHP: Best for people who need strong daily structure, frequent therapeutic contact, and close monitoring while returning home at night.
- IOP: Often a fit for working adults and students who need meaningful support several days a week but can’t step out of life completely.
- Standard outpatient: Better for people with more stability, lower acute risk, or those stepping down after a more intensive phase.
What treatment should actually include
A treatment schedule alone doesn’t solve alcohol use. The content matters. Strong outpatient care usually includes individual therapy, group therapy, relapse prevention work, and practical planning around triggers, routines, and accountability.
Medication can also matter. For some people, medication support reduces cravings or helps them stabilize early recovery without the chaos of repeated stop-start attempts. When anxiety, depression, or other mental health symptoms are part of the picture, treatment also needs to address those directly.
Recovery tends to hold when the program treats the drinking problem and the reasons the person kept returning to alcohol.
Why peer support still matters
Clinical care and peer support shouldn’t be treated like opposing options. They often work best together. A Stanford analysis of 35 studies found that Alcoholics Anonymous was 60% more effective than psychotherapy at achieving sustained abstinence. That doesn’t mean therapy has no value. It means community, repetition, accountability, and shared experience are powerful recovery tools.
For many people, the strongest setup looks like both. Structured therapy helps identify patterns and build skills. Peer support helps the person practice sober living in real life, week after week.
What local fit looks like in practice
A Dallas-area professional might need evening treatment hours. A parent in Euless may need a program that allows them to return home each night. A college student may need care that supports sobriety without removing them from classes altogether.
One local option is Maverick Behavioral Health, which provides outpatient care across PHP, IOP, and standard outpatient levels, along with dual diagnosis services and medication-assisted treatment. The important point isn’t the name of a program. It’s whether the plan is customized for the person’s risk, schedule, and mental health needs.
Questions worth asking before enrolling
Before starting a program, a person should get clear answers to a few issues:
- How often will therapy happen
- What happens if cravings spike or relapse occurs
- How is mental health addressed alongside alcohol use
- Are family involvement and aftercare part of the plan
- Can the schedule work with employment or school
The right treatment program should feel structured, realistic, and specific. If a person in Dallas or Euless wants help sorting through those options, calling (888) 385-2051 is a practical next step.
Building a Sober Life with New Coping Skills
Stopping alcohol is one task. Living without it every day is another. Many people know how to white-knuckle through a few days. Fewer know how to handle stress at 6:30 p.m., a tense dinner, a lonely hotel night, or a weekend invitation that used to revolve around drinking.
That gap is where coping skills matter. Not generic advice. Specific replacements.
Replace the job alcohol was doing
Alcohol usually serves a purpose before it becomes a problem. It may shut off stress, soften social anxiety, fill empty time, numb anger, or signal that the workday is over. A person trying to learn how to stop drinking alcohol has to identify that function first.
A few examples:
- If drinking was a shutdown button after work: create a transition ritual that happens immediately on getting home
- If drinking was social armor: prepare one or two simple responses before events
- If drinking was a boredom fix: schedule something active or absorbing during the highest-risk hours
Without that replacement, the mind keeps returning to the same solution it already knows.
Use support that exists outside the home
Isolation makes cravings louder. Support makes them easier to interrupt. The National Institute on Alcohol Abuse and Alcoholism guidance on treatment and mutual-support groups notes that combining healthcare interventions with Alcoholics Anonymous enhances recovery outcomes and reduces relapse rates. AA also has over 2 million members worldwide, which matters because people often need support at odd hours, not just during appointments.
That scale matters less than the practical benefit. Meetings are accessible, peer-led, and built around repetition. A person can have a rough day, go to a meeting, listen, talk, and leave less alone than they arrived.
Skills that work better than raw willpower
A sustainable daily toolkit often includes:
- Urge interruption: leave the room, change location, call someone, or put time between the urge and the action
- Stress discharge: walking, exercise, journaling, prayer, breathing practice, or a basic routine that settles the body
- Social planning: drive separately, keep an exit plan, and decide in advance what to say if offered a drink
- Evening structure: many relapses happen in unplanned hours, not dramatic moments
For people who need more structured strategies, these coping skills for addiction recovery offer practical ideas that can be used alongside therapy and support groups.
Sobriety gets stronger when a person stops asking, “How do I avoid drinking forever?” and starts asking, “What do I do instead tonight?”
Expect discomfort without treating it as failure
Early sobriety can feel flat, restless, and emotionally uneven. That doesn’t mean it isn’t working. It often means the nervous system is adjusting and the person is learning to live without a chemical shortcut.
The goal isn’t to feel amazing every day. The goal is to keep building a life where alcohol is no longer the automatic answer.
Your Aftercare Plan for Long-Term Relapse Prevention
Many people focus hard on quitting and then underestimate what comes next. That’s where relapse often enters. The risk isn’t only the first sober weekend. It’s the slow return of stress, overconfidence, untreated anxiety, relationship conflict, exhaustion, and the belief that the problem is now fully handled.
That’s why aftercare isn’t optional. It’s part of treatment, not something extra added if there’s time. According to the Harvard Health page cited in the verified data, 70% of relapses happen in the first year, and 50% of people with alcohol use disorder also have anxiety or depression. The same source notes that integrated outpatient programs using CBT and MAT lowered relapse by 45% over 12 months compared with self-help alone.
What a strong aftercare plan includes
A useful aftercare plan usually has several parts working together:
- Continued therapy: especially when stress, trauma, anxiety, or depression drive the urge to drink
- Ongoing group connection: regular peer support keeps recovery visible and accountable
- Trigger review: the person should know their highest-risk people, places, emotions, and time windows
- A response to slips: one drink or one bad night should trigger action, not disappearance
Working professionals need a plan that matches real life
For adults in Dallas-Fort Worth, relapse risk often builds in ordinary routines. Travel, client dinners, late commutes, irregular sleep, and private stress can all reopen old patterns. A strong aftercare plan has to fit those realities or it won’t hold.
Relapse isn’t proof that treatment failed. It usually means the plan needs to be tightened, extended, or better matched to the person’s actual life.
The same is true for people with dual diagnosis. When alcohol and mental health symptoms feed each other, recovery tends to last longer when both are treated together instead of in separate lanes.
Your journey to a healthier life is possible, and you don’t have to do it alone. Call the compassionate team in Euless, TX at (888) 385-2051 to create a personalized aftercare plan.
If alcohol has started to control daily life, waiting usually makes the next step harder. Maverick Behavioral Health provides outpatient substance use and mental health treatment for adults in Euless, Dallas, and the surrounding DFW area, including PHP, IOP, standard outpatient care, dual diagnosis treatment, and medication-assisted support. Call (888) 385-2051 for a confidential conversation about safe next steps and treatment options that fit real life.