


A lot of people land here after the same uneasy realization. Lorazepam helped at first. It calmed panic, eased sleepless nights, or got someone through an overwhelming stretch. Then the prescription kept going, the refill routine became normal, and now there's a new question in the room: why does it feel harder to function without it, and why do the side effects seem more serious than anyone expected?
That concern is valid. For many patients and families, the issue isn't misuse in the way people often imagine it. It's that a medication meant to provide short-term relief can gradually create long-term problems of its own. When that happens, the side effects are no longer just “annoying.” They're signals that the treatment plan needs to be re-evaluated carefully, with medical support and a realistic plan.
Table of Contents
- From Short-Term Relief to Long-Term Concern
- Why Lorazepam Is Not a Long-Term Solution
- Cognitive and Physical Effects of Chronic Use
- The Unseen Cycle of Dependence and Withdrawal
- High-Risk Interactions and Psychiatric Dangers
- A Safe Path Forward How to Taper Lorazepam Correctly
- Find Tapering Support and Care in Euless and Dallas
From Short-Term Relief to Long-Term Concern
Lorazepam can feel like a lifeline when anxiety is intense or sleep has fallen apart. That early benefit is real. A calmer body and a quieter mind can make it seem like the medication is finally fixing the problem.
But long-term use changes the equation. Families often start noticing subtle signs first. A loved one seems foggier. Reactions are slower. Anxiety between doses feels sharper. Sleep may not stay better. Daily life starts revolving around avoiding discomfort rather than building stability.
That's why questions about Lorazepam side effects long term deserve a direct answer. The concern isn't only sedation. The bigger issues are dependence, withdrawal, memory changes, slower thinking, safety problems, and the possibility that the medicine is no longer helping enough to justify the risk.
The medication can start acting less like a bridge and more like something the brain has to work around.
A careful review matters because these problems are treatable. The next step usually isn't panic, shame, or abrupt stopping. It's an informed reassessment. For some people, that means confirming the medication still has a clear role. For many others, it means building a safer path that addresses the original anxiety or insomnia without leaving the person trapped in a cycle of worsening side effects.
Why Lorazepam Is Not a Long-Term Solution
Lorazepam belongs to the benzodiazepine family. These medications can reduce acute anxiety fast, but they were never designed to carry the whole burden of long-term treatment. The core reason is neuroadaptation. Over time, the brain adjusts to the presence of the drug.

The FDA's official lorazepam labeling states that there is no evidence from systematic clinical studies to support its effectiveness for use longer than 4 months, which is a critical limitation when a prescription has stretched well beyond that window (FDA lorazepam labeling on duration of effectiveness). The same label notes there is no evidence of accumulation with administration for up to six months, which points clinicians toward the underlying chronic problem. It isn't drug buildup. It's the brain adapting in ways that lead to tolerance, dependence, and withdrawal.
How the shift happens
At the start, lorazepam can reduce symptoms quickly. With ongoing exposure, the nervous system compensates. That adaptation can make the same dose feel less effective, and it can leave the person more vulnerable to rebound anxiety or sleep disruption when the medication wears off.
This matters for families because the pattern is often misunderstood. A person may believe their anxiety disorder is suddenly “getting worse,” when part of what's happening is the body struggling with long-term benzodiazepine exposure. That isn't a character flaw, poor motivation, or a failure of willpower. It's a predictable physiologic response.
A better long-range plan usually includes treatment that does more than suppress symptoms for a few hours at a time. For people trying to understand options beyond medication-only care, resources on personalized anxiety therapy in Kelowna can help illustrate what individualized anxiety support looks like in practice.
What works better over time
Long-term improvement usually comes from matching the treatment to the problem. Panic, generalized anxiety, trauma-related symptoms, and insomnia don't all respond to the same strategy. When lorazepam has become a long-term habit, the more effective approach is often to reassess the diagnosis, review current functioning, and build a taper plan if risks now outweigh benefits.
Practical rule: If a medication meant for short-term relief has become necessary just to feel normal, the treatment plan needs a fresh clinical review.
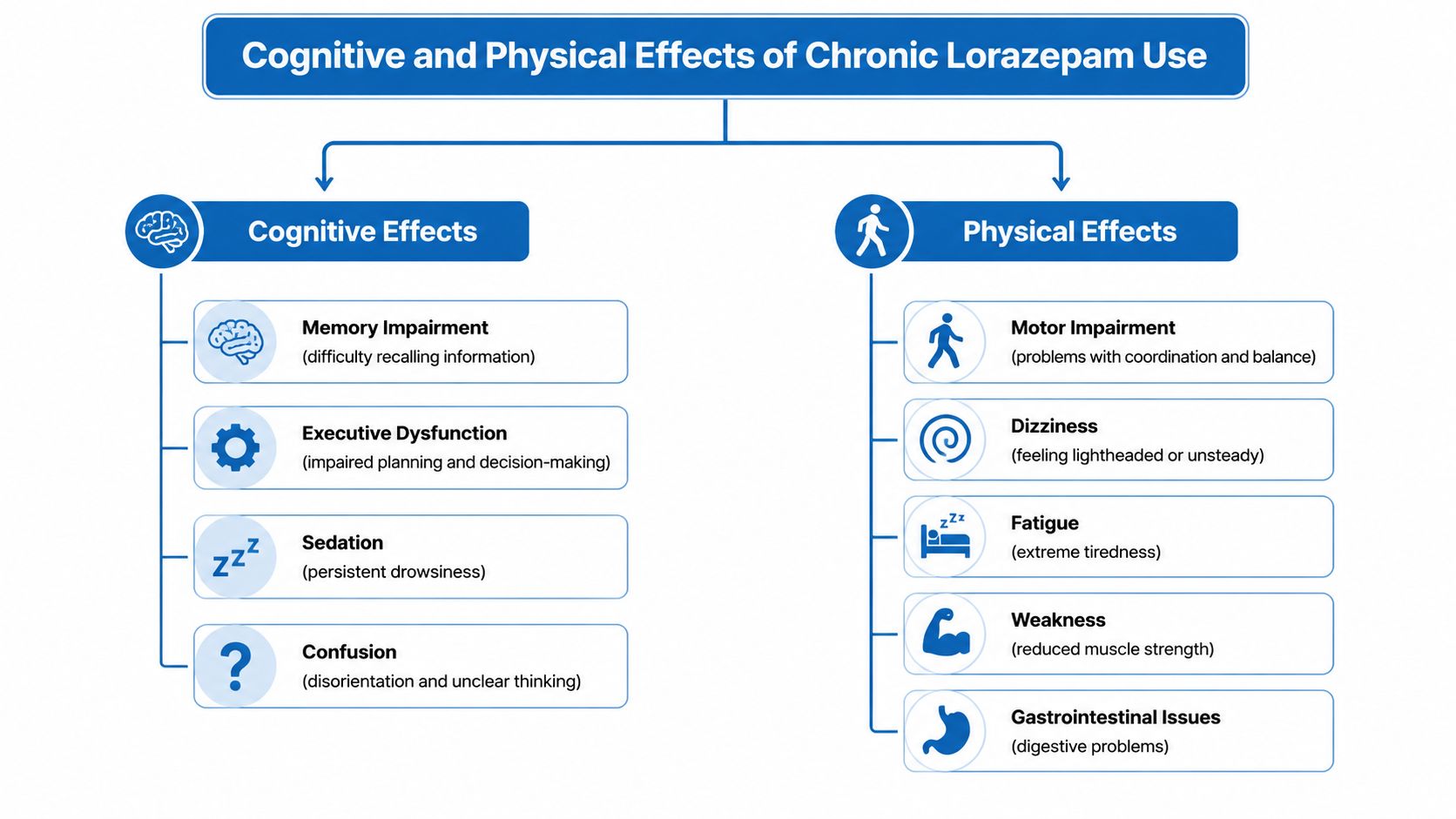
Cognitive and Physical Effects of Chronic Use
Many people asking about long-term lorazepam side effects aren't looking for a textbook list. They want help making sense of changes they can see: forgetfulness, slowed reactions, unsteadiness, fatigue, and a general sense that the person isn't functioning like themselves.
A placebo-controlled study in older long-term lorazepam users found that an acute oral dose of their usual medication caused poorer recall and slower psychomotor performance than placebo, with measurable effects lasting up to 5 hours after dosing. The same evidence summary notes that benzodiazepines are associated with driving impairment comparable to a blood alcohol level of 0.050% to 0.079%, and increase hip-fracture risk in older adults by at least 50% (study summary on memory, psychomotor function, driving risk, and hip fracture risk).
Cognitive problems that affect daily life
The cognitive side of chronic lorazepam use often gets minimized because it can look subtle at first.
- Memory disruption can show up as repeated questions, forgotten appointments, or trouble recalling recent conversations.
- Slower processing can make work tasks take longer, especially anything involving attention shifts, multitasking, or quick decisions.
- Mental fog may feel like trying to think through a heavy blanket. The person is awake, but not fully sharp.
- Reduced judgment under stress can make ordinary decisions harder, especially when anxiety is already part of the picture.
For older adults, these changes can blend into concerns about aging or early cognitive decline. That's one reason families sometimes miss the medication's role. If someone seems more confused, less steady, or less able to track details than they used to, the drug list needs a close review.
Physical risks that families often notice first
The physical effects are often easier to spot than the cognitive ones.
| Concern | What it may look like in real life |
|---|---|
| Poor coordination | Bumping into furniture, hesitation on stairs, trouble with fine motor tasks |
| Sedation | Napping more, slowed speech, low energy, reduced alertness |
| Balance problems | Swaying, near-falls, fear of walking unassisted |
| Delayed reaction time | Slower braking while driving, slower responses in busy environments |
These effects matter outside the home too. A person may still be legally driving, still going to work, and still appearing “functional,” while their actual reaction time and attention are compromised in ways that increase risk.
Chronic stress can create fatigue on its own, so it helps to separate medication effects from the body's stress response. For readers sorting through that overlap, this resource on addressing persistent fatigue from stress offers useful context.
A common mistake is assuming long-term use means the body has “gotten used to it” enough that impairment is no longer clinically important. The available evidence does not support that reassurance.
The Unseen Cycle of Dependence and Withdrawal
One of the hardest parts of long-term lorazepam use is that the medication can create the very crisis that keeps it in place. The person takes it to reduce anxiety or help sleep. Then the body adapts. If the dose drops or a refill is delayed, distress appears quickly, and it feels like proof the medication is still needed.
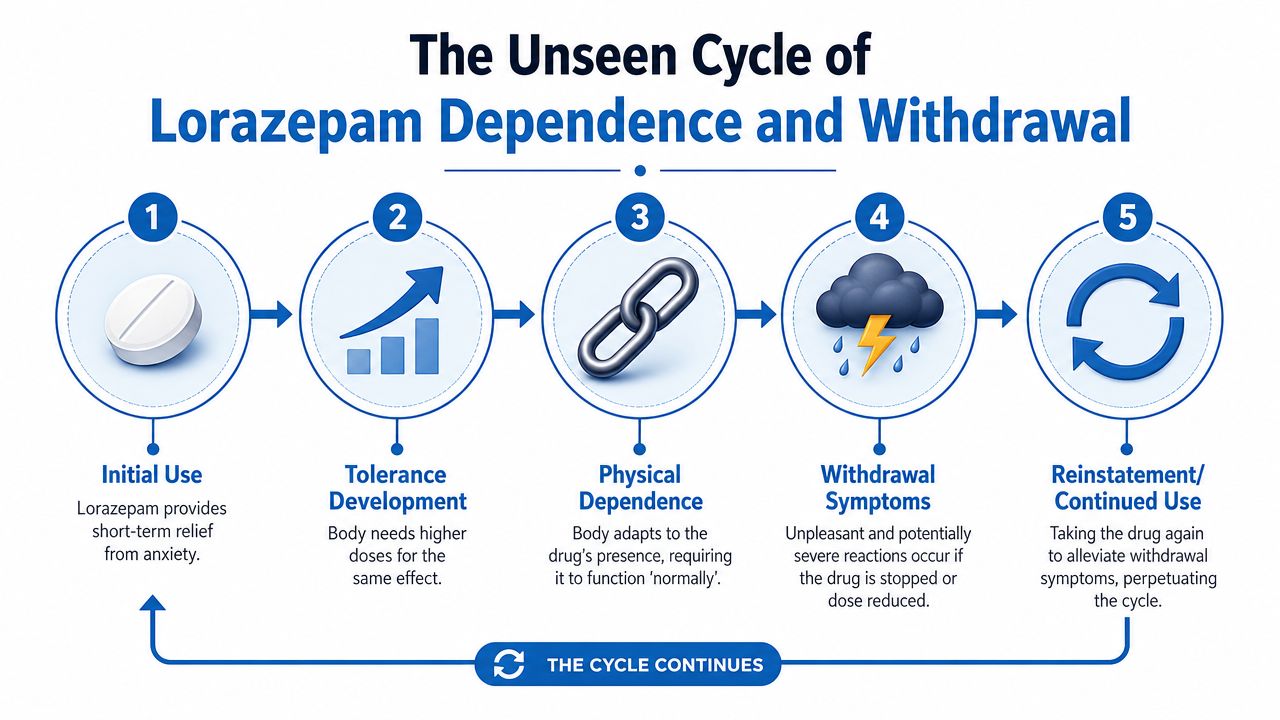
Dependence is not the same as addiction
Physical dependence means the body has adapted to the medication's presence. That can happen even when someone takes lorazepam exactly as prescribed. Addiction involves a broader pattern of compulsive use despite harm. The distinction matters because many patients develop dependence without seeing themselves in the word “addiction,” which can delay getting help.
The American Academy of Family Physicians notes that withdrawal symptoms from benzodiazepines can appear after only one month of daily use. For lorazepam specifically, withdrawal may begin 6 to 8 hours after the last dose, usually lasts 4 to 5 days, and may peak on day 2 (AAFP review on benzodiazepine withdrawal timing and risks). That timeline helps explain why people can feel abruptly worse between doses or after trying to stop on their own.
What withdrawal can look like
Withdrawal doesn't always begin with dramatic symptoms. Sometimes it starts with a familiar complaint that seems deceptively ordinary.
- Rebound anxiety can feel stronger than the original anxiety problem.
- Insomnia often returns fast and can be severe enough to push the person back to the medication.
- Irritability and agitation can strain relationships and create conflict at home.
- Tremor, sweating, and autonomic symptoms can make people think they're having another medical problem.
- Seizures are a serious risk with abrupt cessation.
The most important practical point is simple. A person can become trapped in a loop where taking lorazepam relieves symptoms caused partly by lorazepam withdrawal. That loop is one reason abrupt stopping goes badly so often.
Stopping suddenly isn't a test of strength. It's a medical risk.
Families should also know that fear of withdrawal is not overreaction. It's often based on prior attempts that went poorly. When someone says, “I tried to cut back and felt awful within hours,” that statement deserves clinical attention, not dismissal.
High-Risk Interactions and Psychiatric Dangers
Long-term lorazepam risk doesn't stop at sedation or dependence. The danger rises sharply when it's combined with other substances that slow the central nervous system, and some patients also develop psychiatric complications that families don't immediately connect to the medication.
The combinations that create the most danger
The FDA warns that combining benzodiazepines with opioids can cause profound sedation and respiratory depression. Alcohol also raises overdose risk with lorazepam. In outpatient care, this isn't an abstract concern. It shows up in common real-world patterns such as taking a prescribed benzodiazepine, drinking in the evening to “take the edge off,” or mixing sedating medications from different prescribers.
A few situations deserve immediate attention:
- Alcohol with lorazepam increases overdose danger and can worsen disinhibition and impaired judgment.
- Opioids with lorazepam create a high-risk combination because both can suppress breathing.
- Other sedating medications can add to confusion, falls, and dangerous oversedation.
- Using extra doses during emotional distress can shift a prescribed medication into an unsafe pattern fast.
People who want a broader look at how another sedative-hypnotic is regulated and why control status matters can review this discussion of whether Ambien is a controlled substance.
When the medication starts worsening mental health
A 2024 pharmacovigilance study found that lorazepam reports were disproportionately associated with drug abuse, suicide attempt, delirium, and psychotic disorder, which is an important reminder that chronic risk can include serious neuropsychiatric destabilization, not just drowsiness (2024 pharmacovigilance findings on lorazepam adverse event patterns).
That finding fits what clinicians worry about in practice. Some patients become more emotionally volatile over time. Others become confused, impulsive, or unusually agitated. In vulnerable people, long-term use can interfere with recovery from anxiety, depression, trauma, or substance use problems by clouding judgment and reinforcing medication-seeking during distress.
When family members notice increasing confusion, agitation, or alarming behavior, the medication list should be reviewed urgently, especially if alcohol, opioids, or multiple sedatives are involved.
A Safe Path Forward How to Taper Lorazepam Correctly
The first rule is direct and imperative. Do not stop lorazepam abruptly without medical guidance. That approach can trigger severe withdrawal and, in some cases, seizures.
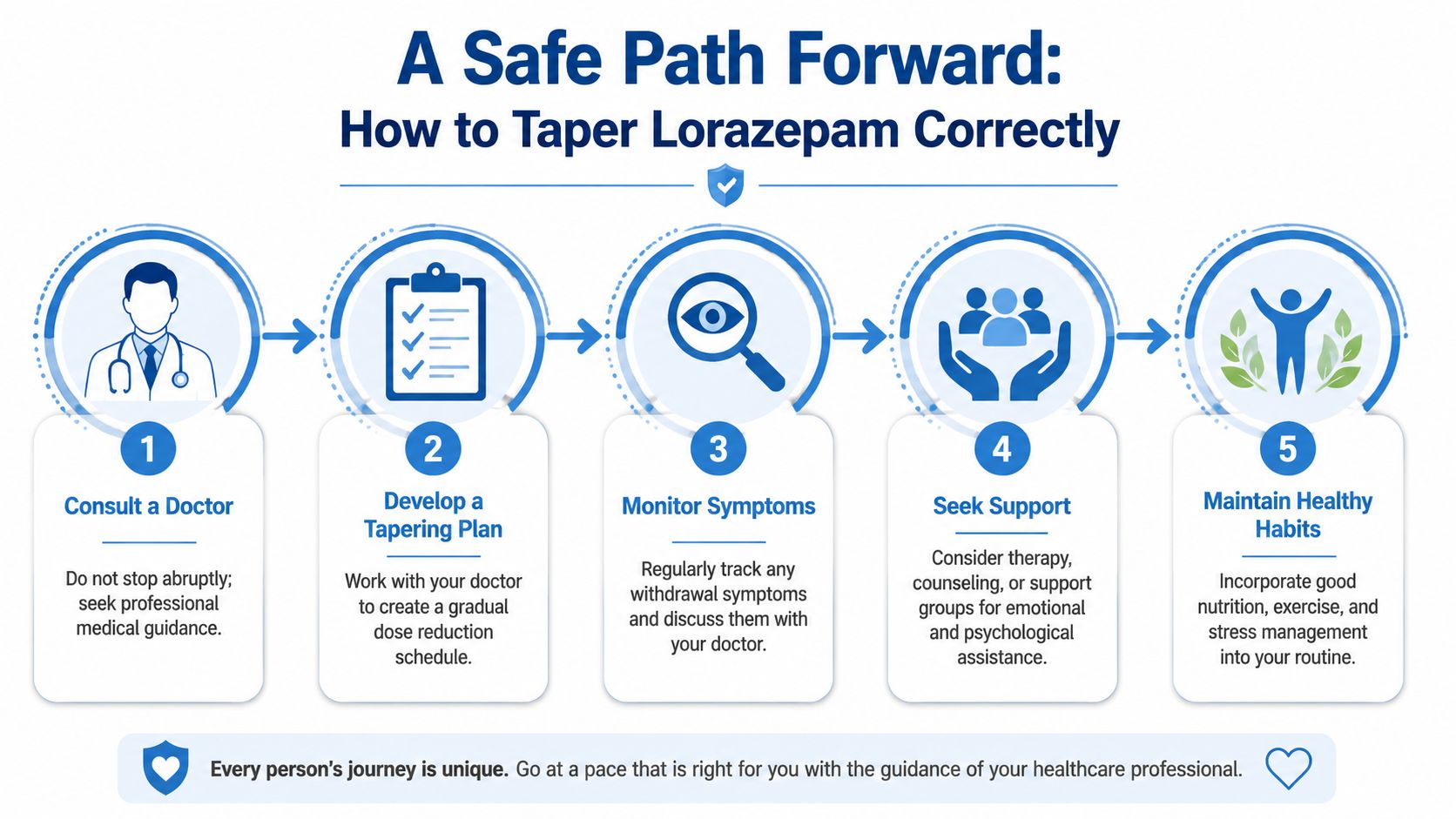
A safe taper works because it gives the nervous system time to adjust gradually. There isn't one universal schedule that fits everyone. The right plan depends on the current dose, how long the person has been taking it, whether alcohol or other substances are involved, past withdrawal history, age, and co-occurring mental health conditions.
What a safe taper usually involves
Most responsible taper plans share a few principles:
Medical assessment first
A clinician reviews the medication pattern, other substances, psychiatric symptoms, sleep issues, and seizure risk.A gradual dose reduction
The aim is to lower the dose carefully enough that withdrawal remains manageable and safety is preserved.Close monitoring
Symptoms are tracked throughout the taper. If confusion, severe anxiety, panic, insomnia, or other complications build too quickly, the plan may need adjustment.Treatment for the original reason lorazepam was prescribed
Anxiety, insomnia, trauma symptoms, or panic don't disappear just because the medication is reduced. Those problems need active treatment during the taper.Support outside medication changes
Therapy, coping skills, sleep routines, and family support can reduce the pressure to return to the drug at the first wave of discomfort.
For readers comparing how structured tapering principles apply in other withdrawal settings, this overview of a Librium taper for alcohol withdrawal can help clarify why gradual, supervised reduction is so important.
What usually does not work
Some strategies sound practical but often backfire.
- Stopping “cold turkey” creates unnecessary risk.
- Making random dose cuts often produces unstable symptoms and panic.
- Using alcohol to soften withdrawal adds danger instead of solving the problem.
- Treating only the withdrawal and ignoring the anxiety disorder leaves the person vulnerable to restarting lorazepam.
The most effective path is usually steady, individualized, and professionally supervised. It may take time, but that time protects the brain and body while creating room for better long-term treatment.
Find Tapering Support and Care in Euless and Dallas
A common situation looks like this. Someone in Euless or Dallas knows lorazepam is causing problems, but they still have to get to work, pick up their kids, sit through classes, and function at home. In that setting, the side effects are no longer just symptoms to endure. They are signs that the treatment plan needs another look, with support that fits real life.

Why outpatient support matters
Structured outpatient treatment can make practical sense in this situation. It allows a person to address long-term lorazepam use while staying connected to daily responsibilities, which is often the difference between starting a taper and postponing it again.
Good outpatient care does more than lower a dose. It reassesses the full picture: why lorazepam was started, what side effects have developed, what symptoms return during a taper, and what mental health support is needed so the person is not left white-knuckling through the process.
At this stage, treatment often works best when it includes several pieces together:
- Psychiatric review to decide whether lorazepam still belongs in the plan and how to reduce it safely
- Mental health treatment for anxiety, panic, trauma, depression, or substance use that may be driving continued reliance on the medication
- Individual and group therapy to build coping skills that do not depend on a benzodiazepine
- Ongoing monitoring so the taper can be adjusted if symptoms become too disruptive or risky
- Aftercare planning to lower the chance of returning to long-term use after the taper ends
Sleep often becomes one of the hardest parts of recovery. A practical resource like this ultimate guide to natural sleep can support conversations about non-drug sleep habits during treatment.
What to do next in the Dallas Fort Worth area
Maverick Behavioral Health provides outpatient substance use and mental health treatment in the Euless and Dallas-Fort Worth area, including PHP, IOP, and standard outpatient care. That type of support can help when long-term lorazepam use is tied to anxiety, depression, other substances, or repeated failed attempts to taper without supervision.
If you are not sure how that structure works, this explanation of what IOP therapy involves gives a clearer picture of the level of support available. For many families, that structure brings relief. It turns a frightening cycle of side effects, dose changes, and setbacks into a plan that can be followed.
If long-term lorazepam use has led to memory problems, sedation, emotional instability, unsafe mixing with alcohol or opioids, or unsuccessful efforts to cut down, it is time to get help. In my experience, waiting usually adds more instability, not more readiness.