


A lot of people search for help with librium taper alcohol withdrawal after a bad night. Someone has tried to cut back or stop drinking, then the shaking starts. Sleep disappears. Anxiety ramps up. A spouse watches for breathing. An adult child wonders whether this is something that can be handled at home or whether it's already dangerous.
That uncertainty matters, because alcohol withdrawal can turn serious fast. The good news is that there is a structured medical approach that helps reduce risk, ease symptoms, and make the process more manageable. For many people in Euless, Dallas, and the broader Fort Worth area, the right answer isn't trying to white-knuckle detox alone. It's getting supervised care and learning how to stop drinking alcohol safely with a plan that fits real life.
Table of Contents
- Navigating the First Step of Alcohol Withdrawal
- Why Librium is a Gold Standard for Alcohol Detox
- How a Librium Taper for Alcohol Withdrawal Works
- Monitoring Symptoms and Critical Safety Red Flags
- Outpatient Taper Support in the Dallas-Fort Worth Area
- Your Path to Lasting Recovery Starts Today
Navigating the First Step of Alcohol Withdrawal
The first step usually doesn't feel brave. It feels frightening.
A person may wake up and realize that not drinking has become its own problem. The body is sweating. Hands won't stay still. The mind is racing. Family members may think this is just anxiety or a hangover, but alcohol withdrawal can be far more serious than that. Trying to stop without medical guidance can put someone in real danger.

What helps many families is learning that detox doesn't have to mean chaos. A Librium taper is a familiar, established medical method used to calm the nervous system while the body adjusts to the absence of alcohol. Instead of letting symptoms surge unchecked, a clinician uses scheduled medication and close monitoring to lower the chance of severe complications.
Why this medication became so important
Librium (chlordiazepoxide) was approved by the FDA in 1960 as the first benzodiazepine, and it became a cornerstone of alcohol withdrawal care because its half-life is approximately 100 hours, creating a self-tapering effect that helps prevent dangerous rebound symptoms such as seizures, according to clinical background on Librium tapering.
That long action is one reason families often hear Librium discussed in detox settings. It doesn't hit and wear off as quickly as shorter-acting medications. For the right patient, under supervision, that can create a steadier landing.
Practical rule: If someone is already having significant shaking, confusion, panic, or a history of severe withdrawal, this is not a do-it-yourself project.
A safe plan also gives people something emotionally important. It replaces guessing with structure. There's a schedule. There's monitoring. There's a clear next step if symptoms change. For someone who has been cycling between drinking to feel normal and trying to stop alone, that structure often brings the first real sense of control in a long time.
What families often get wrong
Families sometimes wait too long because the person seems “mostly okay” between spikes in symptoms. Alcohol withdrawal often doesn't follow a calm, linear pattern. Someone can look stable, then worsen.
A medically supervised taper changes that dynamic. It gives the person a defined path forward and gives loved ones a clear way to respond instead of reacting in fear.
Why Librium is a Gold Standard for Alcohol Detox
Alcohol withdrawal causes the brain and body to enter a hyperactive state. Chronic alcohol exposure suppresses normal nervous system balance over time. When alcohol suddenly disappears, that calming effect vanishes as well, and the system can rebound hard. That's why withdrawal can involve tremors, sweating, agitation, insomnia, increased anxiety, and in severe cases, seizures or delirium tremens.
Librium is often used because it helps calm that overactivation in a measured way. Its long duration gives clinicians room to smooth out the sharp peaks and valleys that make withdrawal dangerous.
What its long action changes in real practice
A short-acting medication can wear off quickly and leave the patient vulnerable to rebound symptoms between doses. Librium's longer presence in the body reduces that risk for many people. In practical terms, this can mean fewer abrupt swings and a more stable taper, which is especially useful when care happens outside a hospital.
That doesn't mean Librium is automatically the right fit for everyone. Good prescribing still depends on the person's withdrawal severity, medical history, liver function, other medications, current substance use, and whether they can be monitored reliably. The medication works best when the treatment setting matches the risk level.
Why clinicians trust it
Clinical guidance commonly includes chlordiazepoxide among the most frequently used benzodiazepines for alcohol withdrawal, and its long-acting profile is one reason it's often preferred for outpatient use. The medication's effect gradually fades instead of dropping off abruptly, which is why many clinicians describe it as forgiving when compared with shorter-acting alternatives.
A Librium taper works best when the schedule is built around symptoms, not around convenience.
The other reason it's considered a gold standard is that it addresses the most dangerous part of withdrawal. Benzodiazepines such as Librium are used because they lower the risk of withdrawal seizures and help prevent progression to more severe states. That protective role is why supervised detox is so different from trying to rest, hydrate, and wait it out.
What works and what doesn't
Some approaches help. Others create unnecessary risk.
- What works: Careful assessment before the first dose, a clear prescribing plan, and regular check-ins during the taper.
- What works: Honest reporting about how much alcohol was used, when the last drink happened, and whether there have been prior withdrawal episodes.
- What doesn't work: Saving pills, doubling up without approval, or using the medication on an irregular schedule.
- What doesn't work: Mixing Librium with alcohol or other sedating substances.
People often focus on whether the medication is “strong.” The better question is whether the treatment is structured. A strong medication without oversight can be risky. A well-managed taper can make a dangerous withdrawal far safer and more tolerable.
How a Librium Taper for Alcohol Withdrawal Works
A Librium taper for alcohol withdrawal is never one-size-fits-all, but the basic idea is simple. A clinician starts with a dose that matches the person's withdrawal severity, then reduces the amount over several days while watching symptoms closely.
Withdrawal severity is often assessed with the CIWA-Ar scale, and while severe withdrawal is typically managed in-patient, moderate outpatient withdrawal may begin with 25 to 50 mg of Librium, with total daily dose and taper length adjusted over 5 to 10 days based on response, as described in guidance on Librium taper protocols.
That range matters because the safest plan depends on the person in front of the clinician. A younger healthy adult with moderate symptoms and strong family support may follow one schedule. Someone with unstable symptoms, repeated withdrawal episodes, or limited supervision may need a higher level of care.
Two scheduling styles clinicians use
Symptom-triggered dosing is common in hospitals and detox units. Staff assess symptoms repeatedly, often using CIWA scoring, and give medication when the patient reaches a certain threshold.
Fixed-dose scheduling is often more practical in outpatient settings. The patient takes set doses at set times, then the amount is gradually reduced. This approach works best when there's reliable follow-up, clear instructions, and a stable home situation.
For many outpatient programs, fixed-dose scheduling is easier to implement because it doesn't require round-the-clock bedside scoring. It also gives patients and families a more predictable routine.
People who want to understand the broader role of medications in recovery often benefit from reviewing medication-assisted treatment in a larger context. Detox medication is only one part of treatment, but it can be a crucial one.
An example outpatient taper table
The table below is only an example. It is not a prescription, not a safe self-detox plan, and not a substitute for medical care. A real taper must be designed by a licensed prescriber.
| Day | Morning Dose (mg) | Afternoon Dose (mg) | Evening Dose (mg) | Bedtime Dose (mg) | Total Daily Dose (mg) |
|---|---|---|---|---|---|
| 1 | 25 | 25 | 25 | 25 | 100 |
| 2 | 25 | 25 | 25 | 25 | 100 |
| 3 | 25 | 25 | 25 | 0 | 75 |
| 4 | 25 | 25 | 0 | 0 | 50 |
| 5 | 25 | 0 | 25 | 0 | 50 |
| 6 | 25 | 0 | 0 | 0 | 25 |
| 7 | 0 | 0 | 25 | 0 | 25 |
This kind of example shows the basic taper logic. Start high enough to control symptoms, then step down as the withdrawal process settles. Some tapers are shorter. Some extend further within that 5 to 10 day window. Some patients need adjustments during the process because symptoms don't follow a neat schedule.
What a patient should expect day to day
The first day is usually focused on stabilization. The prescriber wants to know whether the starting dose is controlling tremor, agitation, sweating, and sleep disruption.
The middle portion of the taper is where close monitoring matters most. If symptoms are improving, doses usually continue to fall. If symptoms break through, the schedule may need adjustment. That is exactly why self-detox is risky. The plan has to respond to the body, not just the calendar.
A family member can help by tracking simple observations:
- Timing: When symptoms get worse and when they improve.
- Function: Whether the person can rest, drink fluids, think clearly, and follow instructions.
- Safety: Any confusion, falls, missed doses, or urge to drink while taking Librium.
A good taper is structured but flexible. A bad taper is rigid, poorly supervised, or based on guesswork.
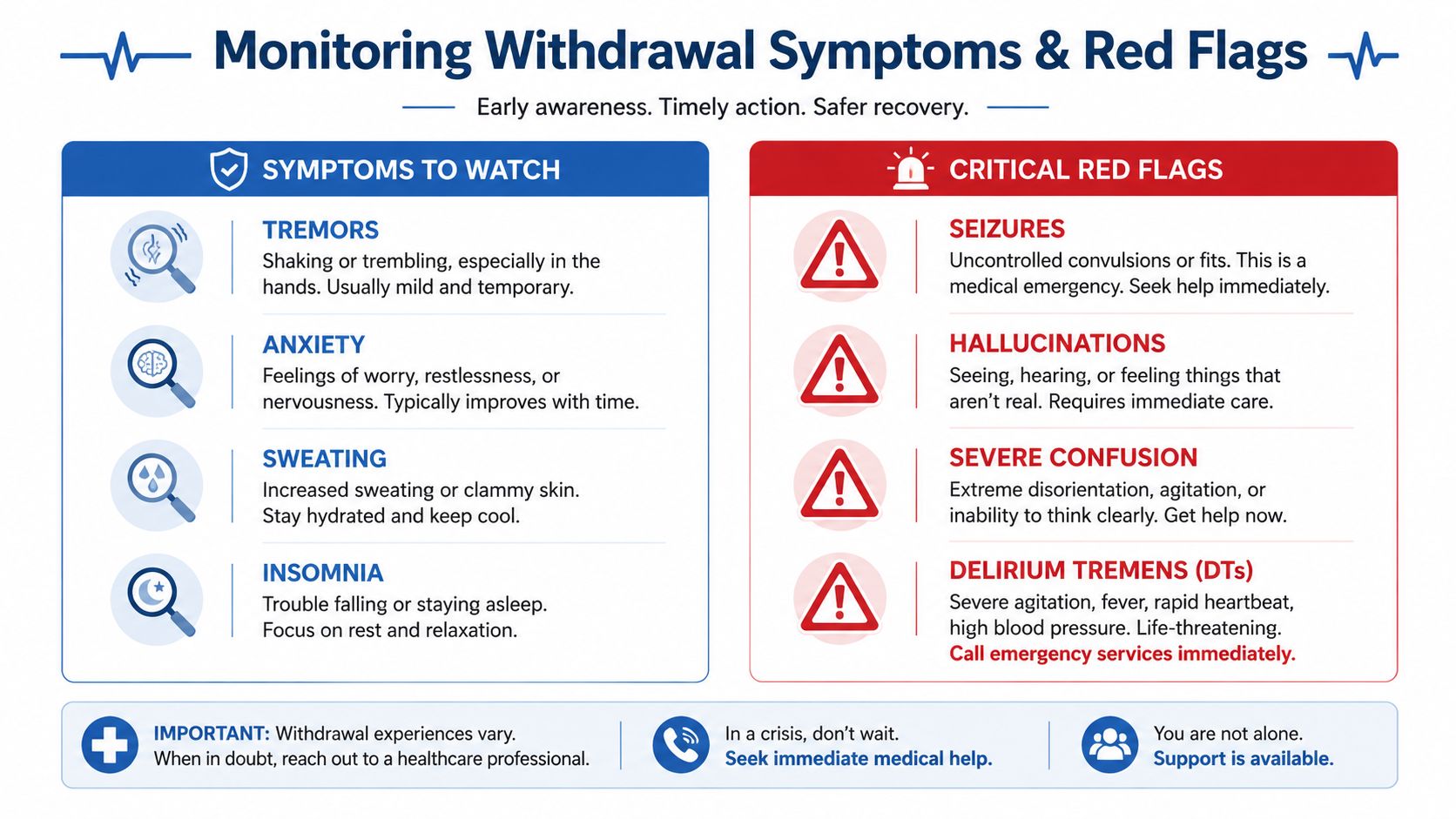
Monitoring Symptoms and Critical Safety Red Flags
The safest families are the ones who know the difference between expected discomfort and a true emergency. Alcohol withdrawal can look messy even when treatment is working, but there are limits. Some symptoms can be watched. Others need immediate escalation.
Expected symptoms during a supervised taper
Even with a well-designed taper, some symptoms can still show up. That doesn't automatically mean the plan is failing.
Common symptoms clinicians often watch for include:
- Tremor: Shaky hands, internal shakiness, or trouble holding objects steadily.
- Anxiety: A keyed-up feeling, panic, or a sense that something is very wrong.
- Sweating: Night sweats, clammy skin, or episodes of sudden perspiration.
- Sleep disruption: Trouble falling asleep, waking often, or feeling exhausted but unable to rest.
- Mild sedation from Librium: Drowsiness, slowed thinking, or feeling unsteady.
These symptoms should still be reported to the treatment team. “Expected” doesn't mean ignored. It means the symptom may be manageable if the person remains oriented, safe, and medically stable.
When it becomes an emergency
Some signs mean the person needs emergency care right away. Family members should not debate these. They should call 911 or go to the nearest emergency room.
Critical red flags include:
- Seizure activity
- Hallucinations, including seeing or hearing things that aren't there
- Severe confusion or inability to recognize people or surroundings
- Extreme agitation that can't be redirected
- Dangerous worsening of tremors with escalating distress
- Falls, passing out, or inability to stay awake safely
If confusion, hallucinations, or seizure symptoms appear, outpatient management may no longer be appropriate.
There is another safety issue people often miss. A taper that becomes too uncomfortable can tempt the person to drink again, take extra doses, or use other sedating substances. That combination can become dangerous quickly.
Why rigid tapers can fail
Responsive clinical oversight matters most in these situations. Expert-led benzodiazepine withdrawal clinics note that when symptoms intensify during a taper, the plan may need temporary dose stabilization or a slower reduction, and rigid schedules that ignore patient feedback have much higher failure rates, according to benzodiazepine tapering guidance.
That principle applies directly to alcohol detox. A printed schedule isn't enough. The clinician has to know what's happening in real time. If the person is over-sedated, doses may need to change. If withdrawal is breaking through, the schedule may need to slow down or the level of care may need to increase.
Families should keep one core rule in mind. If symptoms are escalating and the person looks less safe, the plan needs medical reassessment that day.
Outpatient Taper Support in the Dallas-Fort Worth Area
Most online discussions of librium taper alcohol withdrawal focus on hospitals. That makes sense for severe cases, but it leaves out a large group of people who need help and still have work, school, parenting, or transportation constraints. They need structure, but they also need flexibility.
That gap is real. Most available guidance centers on inpatient CIWA-based detox, while outpatient management remains underexplained, highlighting the importance of specialized outpatient programs that provide frequent check-ins and structured monitoring for people in the Dallas-Fort Worth area who can't commit to inpatient care, as noted in outpatient Librium detox guidance.

What outpatient oversight actually looks like
A safe outpatient taper is not casual care. It should include repeated clinical contact, medication review, symptom monitoring, and a clear plan for when the person needs a higher level of care.
That may involve:
- Frequent check-ins: The treatment team reviews withdrawal symptoms, sedation, sleep, cravings, and any return to alcohol use.
- Medication adjustments: If the patient isn't tolerating the taper, the prescriber can slow reductions or change the approach.
- Therapeutic support: The person isn't only detoxing from alcohol. They're also dealing with fear, stress, family pressure, and often shame.
- Dual diagnosis care: Anxiety, depression, trauma, and alcohol misuse commonly overlap. Treating only the withdrawal leaves major relapse drivers untouched.
People exploring recovery options often also need practical coping support between visits. For some, simple tools to manage anxiety can help organize what symptoms are emotional distress, what symptoms may be withdrawal-related, and what should be reported to the treatment team right away.
Why local flexible care matters
Outpatient treatment has to fit daily life or people won't use it. A working adult in Euless may not be able to disappear into a hospital for several days. A college student in Dallas may be trying to protect classes and housing. A parent in Fort Worth may need care that allows them to remain engaged at home while still receiving clinical supervision.
That's where structured programs such as PHP and IOP become practical. They create a middle path between doing nothing and requiring full hospitalization. People can learn more about outpatient drug rehab if they're trying to understand how that level of care works in real terms.
Outpatient care works when the patient is medically appropriate for it, has reliable follow-through, and can be monitored closely enough to catch changes early.
The trade-off is straightforward. Outpatient care offers flexibility, but it demands honesty, attendance, and responsiveness. If someone misses check-ins, keeps drinking, or develops red-flag symptoms, that flexible model stops being safe. When used well, though, it can give people in the Dallas-Fort Worth area a realistic way to start treatment without putting the rest of life completely on pause.
Your Path to Lasting Recovery Starts Today
A Librium taper can make alcohol withdrawal safer, but detox is only the opening move. It helps stabilize the body so the person can think clearly enough to start actual recovery work. Without that next phase, many people end up right back in the cycle that brought them here.
Detox is the beginning, not the whole treatment
Some people will need inpatient detox instead of outpatient support. That's often the safer choice when withdrawal is severe, when there's a history of seizures or delirium tremens, when the home setting is unstable, or when other medical and psychiatric problems are complicating the picture.
For others, structured outpatient treatment can be the right step after medical evaluation. That setting allows ongoing therapy, relapse prevention planning, family support, and treatment for co-occurring mental health symptoms. It also gives people a better chance to build routines that still work once the taper ends.
Recovery often becomes more sustainable when treatment is accessible. That's one reason many people also look into flexible models in other areas of addiction care, including resources discussing telehealth for opioid dependence in Pennsylvania. The delivery model may differ, but the principle is the same. People do better when care is structured, consistent, and practical enough to keep using.
The next right step
No one needs to prove how sick they are before asking for help. If alcohol withdrawal is already causing shaking, fear, sleeplessness, sweating, or confusion, the safest choice is to get assessed now. Waiting for things to become unmistakably severe is a gamble.
A medically supervised librium taper alcohol withdrawal plan can reduce risk. The right outpatient program can add monitoring, accountability, and therapy. That combination is what turns a crisis into a starting point.
If alcohol withdrawal has started, or if stopping drinking feels dangerous, Maverick Behavioral Health offers confidential help for adults in Euless, Dallas, and the surrounding Dallas-Fort Worth area. Call (888) 385-2051 to speak with a team member about assessment, outpatient options, and the safest next step toward recovery.